The DSM-V-TR and many psychopathology texts group Somatic and Dissociative disorders together. In the DSM-V-TR somatic disorders are listed after dissociative disorders which are tied to stress and PTSD. They both share created realities that are not true but they also differ in direction. Somatic disorders attach to physical symptoms without no correlating reality or pathology from a physical sense but find their origin in the mind. Likewise, many are tied to anxiety, or fear of possessing the actual disease associated with the symptoms. Dissociate disorders are tied to breaks from reality that do not exist as well but more so in the mind and one’s surroundings. They are tied to trauma and stress. This leads to derealization and depersonalization, various amnesias and dissociative identity stemming from trauma. In this short blog, we will review the basis and criteria of diagnosis for different somatic disorders as well as dissociative disorders.
Somatic disorders contain symptoms of a disease created by the mind with no real existence of the disease within the person. Somatic means coming from the mind and manifesting physiological manifestations of a particular physical disorder (Barlow, et, al., 2023). Similar to Somatic Symptom Disorder is Conversion Disorder. Freud believed that the energy associated with mental illness could manifest as physical disease in other parts of the body causing motor control issues that were only a product of the mind (Barlow, et al., 2023).
Hypochondria or Illness Anxiety Disorder can leave a person impaired socially constantly seeking professional and medical help costing the health system millions of dollars
The biggest difference between Somatic Disorder and Conversion Disorder was the the type of physical manifestation and mental state. In Somatic Disorder there are a broad range of persistent physical disorders including pain and fatigue. These irks and pains cause discomfort throughout the day and lead to intense anxiety within the individual as the person attempts to understand the nature of their illness. Conversion differs in the manifestation and reaction. The manifestation effects motor control and cause paralysis, blindness, or other body movement. It usually follows an immediate stressor and can resolve itself quicker. Hence individuals do not deal with it longer over a chronological period (DSM-V-TR, 2022).
The DSM-V-TR lists these criteria Somatic Symptom Disorder for diagnosis .
A. One or more somatic symptoms that cause significant disruption in life
B. Excessive thoughts or behaviors tied to the somatic symptoms with at least one of the following:
1. disproportionate and persistent thoughts about the seriousness of the issue
2. high levels of anxiety about the symptom or overall health
3. excessive time and energy directed to these symptoms and concerns
C. These symptoms persist for 6 months.
Somatic Symptom Disorder can be specified with predominant pain, persistent symptoms, and as mild, moderate or severe.
(DSM-V-TR, 2022).
The DMS-V-TR lists this criteria for Conversion diagnosis
A. One or more of the symptoms have altered motor or sensory function
B. Clinical findings discover no correlation between the symptoms and recognized neurological disorder
C. There is no rational explanation for the disorder
D. The symptom causes clinically significant distress or functioning
It can be specified as acute, chronic, with psychological or without psychological stressor, with various symptom types such as weakness or paralysis, abnormal movement, swallowing symptoms, speech symptoms, seizures, sensory loss, special sensory loss or mixed symptoms.
(DSM-V-TR, 2022).
Another Somatic related disorder is Illness Anxiety Disorder which deviates from Somatic Symptom Disorder in regards to mild to no symptoms with the fear of disease existing in the mind. In the past it was referred to as Hypochondria (Barlow, et al., 2023). The DSM-V-TR lists the following diagnostic criteria for IAD.
A. Preoccupation with having a serious illness
B. Somatic Symptoms or not present or very mild. Other symptoms related to a different disorder are ignored.
C. High level of anxiety about health
D. The individual performs excessive health related behaviors for checkups
E. Illness preoccupation exceeds 6 months
F. The illness preoccupation has no other mental health disorder explanation
The DSM-V-TR specifies them as either care seeking or care avoidant
Ultimately within all of these disorders, individuals refuse to believe experts and fall more so upon their own anxiety ridden logics. They tend to seek their own information and insist they know more than medical professionals.
Tied closely to this are other disorders resulting in faking symptoms or purposely re-creating the symptoms for medical help or attention. Some do this for mental reasons, while others seek financial reward via malingering. Obviously those who seek medical attention and cause symptoms for no logical or financial reason suffer a deeper issue. Factitious Disorder results in this deception to gain attention or aid. Some may also look to keep attention on a person under one’s care by causing or lying about symptoms. In the past this was referred to as Munchausen Syndrome (Barlow, et al., 2023).
It is interesting to see the power of the mind to cause physiological symptoms. Yet if one simply realizes the power of worry to cause a stomach ache, then one can see on a large scale how somatic symptoms can manifest in individuals with greater anxiety and distorted beliefs about health.
Dissociative Disorders
Dissociative Amnesia can be general or selective
While the mind can create physiological symptoms, it can also create separations from reality due to traumatic events or high levels of stress. Many of the dissociative disorders are closely tied to PTSD and trauma induced orders and directly follow the DSM-V-TR’s chapter on Trauma and Stress Related Disorders. The DSM-V-TR points out that many dissociative disorders are frequently in the aftermath of severe trauma. Their symptoms include “unbidden intrusions into awareness and behavior, with accompanying losses of continuity in subjective experiences (2022). This leads to depersonalization, derealization, amnesia and dissociative identity. They can all play roles in the more general umbrella of PTSD but also be a diagnosis within itself.
Depersonalization/Derealization Disorder
According to the DSM-V-TR, depersonalization is the experience of unreality, detachment or being outside or external from one’s own thoughts, or feelings or even sensations of the body. One senses a distorted senses of time and feels absent from self as if almost outside of one’s own body (2022). Similar and also shared frequently between the two is the subjective experience of derealization. Within derealization one experiences unreality and detachment from one’s surroundings as if reality is dreamlike or foggy or distorted (2022).
Dissociative Amnesia
Loss of memory due to trauma leaves the person with an inability to recall or remember. The loss of memory can be localized or selective only to the event, or in more severe cases generalized and effecting one’s identity (DSM-V-TR, 2022). In some cases, it can be specified with dissociative fugue where the individual travels or wanders and cannot relate where they came from (2022).
Dissociative Identity
Dissociative Identity Disorder, formerly known as Multiple Personality Disorder, is a trauma reaction usually formed in early childhood after a traumatic event
One of the most wild and bizarre forms of dissociation is multiple personalities. The DSM-V-TR now labels it as Dissociative Identity in which the person creates different identities when faced with intense trauma. These identities are formed at a younger age and usually add new ones as the person needs to adjust to the unresolved trauma. The DSM-V-TR lists the following criteria for diagnosis
A. Disruption of identity by two or more distinct personality states. The disruption marks a distinct discontinuity in sense of self which displays changes in behavior, memory, perception, consciousness, cognition and sensory-motor functioning.
B. Recurrent gaps to recall events and personal information are inconsistent with normal forgetfulness
C. The symptoms cause significant distress to all elements of social functioning
D. The disturbance is not part of a cultural or religious practice
E. The disturbance is not associated with other substances or medical conditions
(DSM-V-TR, 2022).
Barlow states that most experience an average of 15 different personalities or alters. These alters merge from the host identity (2023). It is believed that under severe cases of trauma, younger children who may possess a genetic and biological vulnerability can develop DID. Diagnosing DID should be done with great care as not to lead an individual to bias or place falsememories regarding a person’s past. Ultimately, it is very difficult to fake DID although criminals in the past have attempted to use a DID defense (Barlow, et, al. 2023).
Some identities are classified as possessive identities which can be mistaken for demonic manifestation. If existing within the religious traditions, one must be careful of cultural and religious beliefs regarding this. In fact, the Catholic Church goes to great lengths and diagnosis within itself to determine a difference between a possessing identity with what it considers to be an external source in its manual of exorcism. Obviously before the era of modern science, many DID were considered possessions and did not meet the current diagnosis within the Catholic Church. Those who are not religious still doubt any form of possession within itself but that is a debate for another day.
Conclusion
Please also review AIHCP’s Healthcare Certifications as well as its Trauma Informed Care program
Physiological symptoms can be very real. The brain can shut itself off for its own defense and create different realities. These are all things that modern psychology has discovered. Many of these issues stem from trauma, anxiety and stress. When a person has the biological vulnerability, the recipe for the manifestation for these disorders become a reality for the person. Therapy and medication can play large roles in facing past issues and traumas. With the exception of DID, many of these mental issues can resolve quickly with proper care. Obviously DID deals with a far deeper trauma and requires deeper psychotherapy to unify the person. That involves identifying triggers, reliving trauma, and carefully realigning the past without causing more damage (Barlow, et al., 2023).
Please also review AIHCP’s Behavioral Health Certifications. AIHCP offers Trauma Informed Care as well for professionals seeking additional training and credentials in this field.
Additional Blogs
Disruptive and Impulse Control Disorders. Access here
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorder” DSM-5-TR (5th ed., text revision). American Psychiatric Association Publishing.
Barlow, D.H., Durand, V.M., & Hofmann, S.G. (2023). Psychopathology. An integrative approach to mental disorder (9th ed.). Cengage Learning
Additional Resources
Goodman, B. 2024. “Somatic Symptom and Related Disorders”. WEBMED. Access here
“What is Somatic Symptom Disorder?” APA. Access here
Healthcare organizations are stretched thin. Everyone wants better outcomes, shorter waits, care that actually feels personal, and they’re supposed to deliver all of it with less money and fewer hands on deck. Nearly a third of what the US spends on healthcare goes to paperwork and administration, not care itself. That number alone tells you where the slack is.
This is the gap AI has quietly started filling by handling the grunt work behind it. Getting schedules right. Catching staffing shortfalls before they turn into a bad week on the floor. Keeping patients moving through the system instead of stuck in a queue. That’s what this blog is actually about: not the sales pitch version of AI in healthcare, but what it’s really doing inside hospitals and clinics right now.
Reduced Wait Times
Most scheduling systems still run on fixed time slots — fifteen minutes here, twenty there — with no regard for a patient’s history or how backed up a physician actually is. The result is predictable: some days a doctor’s sitting on dead time, other days the waiting room is standing-room-only. AI-based scheduling tools fix this by actually looking at the data — past appointment patterns, how long treatments really take, who’s overloaded and who isn’t — and use that to build schedules that hold up. The payoff shows up fast: wait times drop by as much as 37.5%, in some cases, and the whole system runs on less wasted capacity.
Revenue Cycle Management
Medical coding is particularly challenging because mistakes can deny claims and delay reimbursements. But HIPAA-compliant EHR solutions provide secure, standardized clinical data, along with AI-enabled features that identify billing codes to reduce such errors. These solutions also analyze claim history and identify submissions with a higher likelihood of rejection before they are sent to payers.
Smooth Healthcare Experience
When patients cancel scheduled appointments, AI systems can automatically identify those in the queue and offer them newly available time slots. In this way, timely appointment replacements reduce patient waiting periods.
Example: Some advanced systems, such as Epic’s predictive scheduling tools and Qventus AI, consider traffic conditions, travel times, and clinic congestion to schedule appointments realistically. Because of this, clinical resources are better utilized, fewer appointments get missed, and both providers and patients benefit from a smoother experience.
Ensuring Staff Availability
With AI, healthcare experts can conduct predictive workforce planning rather than reactive staffing. To do so, AI-enabled tools analyze department visits, seasonal illness patterns, and public health trends. Based on the consolidated data, they forecast patient needs and proactively adjust staffing levels before departments become understaffed during care delivery.
Optimize Staff Allocation
Not every nurse, tech, or physician on staff has the same certifications or years behind them — which sounds obvious, but a lot of scheduling software still treats staff like interchangeable slots on a grid. The better tools don’t.
QGenda’s Advanced Scheduling, for instance, runs on a rules-based engine that actually weighs a physician’s specialty and skill set against what a given department needs before it builds out a schedule. UKG’s Bryte AI takes a similar approach from a different angle — it looks at workforce data and shift patterns to recommend coverage that matches what units actually need against who’s available to do the work.
Patient Flow Management
Administrative operations, particularly in hospitals, are carried out through interconnected systems, where bottlenecks in admissions, scheduling, or discharge can delay care. To manage such issues, AI-run platforms continuously monitor available beds, admitted patients, and discharge timelines. With the help of this information, administrators can predict capacity challenges.
Faster Documentation
Natural language processing systems can assist with clinical documentation by organizing physician notes and converting conversations into structured records. Healthcare professionals spend less time entering information into systems and more time interacting with patients.
Research Analysis: A study published in JAMA (2026) found that clinicians across five academic medical centers who adopted AI scribes reduced documentation time by an average of 16 minutes/day and total electronic health record usage by 13.4 minutes/day. Across large health systems, these savings can free hundreds of clinician hours annually for patient-facing work rather than administrative tasks.
Faster Responses
Virtual assistants now handle the stuff that used to take up a receptionist’s whole shift — appointment reminders, basic scheduling questions — and they do it around the clock, weekends included, without anyone on payroll pulling a night shift.
NHS trusts have already tested this at scale. After rolling out AI-driven communication tools, no-show rates dropped by around 30%, One hospital’s numbers were even more striking: roughly 9,000 additional patients treated over just three months. It’s simply because fewer people were falling through the cracks between booking and showing up.
Fraud Detection & Compliance Monitoring
Fraud doesn’t announce itself. It hides in volume, in the thousands of claims nobody has time to check by hand. That’s where machine learning earns its place. These models sift through transaction after transaction looking for the stuff a person would miss on page one of a spreadsheet: a billing code that shows up too often, patterns that just don’t add up. Compliance teams still make the call, but now they’re chasing down real leads instead of guessing where to start. This means fewer losses slip through, and fewer headaches when regulators come knocking.
Personalized Treatment Planning
Because of genetics, lifestyle, and existing health conditions, every patient responds differently to treatment. AI systems can analyze these factors, alongside outcome-oriented data from similar patient profiles, which in turn help physicians design personalized treatment plans. This approach, often referred to as precision medicine, thus supports treatment and improves recovery rates.
Enhanced Patient Engagement
A generic pamphlet handed out at checkout doesn’t serve any purpose. What actually works is: a medication reminder timed to when someone actually needs it, or follow-up instructions written for their condition. Patients notice the difference. When the information feels relevant, people are more likely to stick with a treatment plan instead of letting it slide. And that steady thread of communication does more than just keep patients on track — it’s often what keeps the relationship between patient and provider from feeling transactional.
Implementation Considerations
Most AI rollouts in healthcare don’t fail because the technology doesn’t work. They fail because the organization wasn’t ready for it — the data was messy, the staff weren’t bought in, or nobody defined what success looked like before go-live. Getting the sequence right matters more than getting the technology right.
Start with the operational problem, not the tool.
Are patients waiting too long?
Is staffing chronically misaligned with demand?
Is administrative work eating hours that should go to patient care?
Naming the actual bottleneck first keeps AI initiatives from becoming solutions in search of a problem.
Next, look honestly at your data. AI models are only as good as the EHR records, scheduling logs, and operational databases feeding them — and in most health systems, that data is inconsistent across departments, if not outright unreliable. This is usually where projects stall, so it’s worth auditing before committing budget. Pilot before you scale.
Pick one department, one workflow, one measurable outcome. Prove it works — or learn why it doesn’t — before rolling it out organization wide. And make sure whatever you build actually talks to your existing systems; a tool that creates a new data silo has just added a problem, not solved one.
None of this works without the people using it. Staff need to understand not just that AI is making recommendations, but roughly how — enough to trust it, question it when something looks off, and use it as an input rather than an oracle.
Pair that with clear governance around data privacy, security, and regulatory compliance, and metrics you’re actually tracking — wait times, scheduling accuracy, claims turnaround, cost per case — so “success” isn’t a vibe, it’s a number you check quarterly.
End Note
Healthcare operations are shifting from reacting to problems to anticipating them. The organizations that get ahead of this aren’t the ones with the flashiest AI vendor — they’re the ones that fixed their data and trained their people first.
About the Author:
Usman Mehmood is a B2B healthcare content writer who creates clear, research-driven content on medical and healthcare topics for professional audiences. He specializes in simplifying complex healthcare concepts, digital health trends, and clinical technologies into accurate, engaging, and easy-to-understand content. With a strong focus on clarity, credibility, and evidence-based information, he strives to produce content that helps readers make informed decisions while building trust and delivering lasting value.
Please also review AIHCP’s Certification program and CE courses see if it meets your academic and professional goals. These programs are online and independent study and open to qualified professionals seeking a four year certification
Personality Disorders are one of the more interesting types of disorders in mental health. They attract the most attention and curiosity about why individuals act the way they do. For the secular mind, it attempts to explain right and wrong, criminality, oddities, and other quirks that step out of bounds within the social structure. As observed in early psychology, it a disorder but the mind still has the ability to possess rationale in its own self. From a religious perspective, it constitutes the reality of brokenness of humanity and how individual acts of deviation can become habitual aspects of one’s personality (McRay, 2016). These disorders distort personality to such an extent to cause inner personal turmoil in one’s feelings towards others and one’s assertion of those feelings outside the norms of one’s cultural context (McRay, 2016). For this reason, many personality orders are not only odd, eccentric, selfish, rude, and withdrawn, but also violent and terrifying to others.
Personality without empathy or ability to properly feel, think and act within the context of its cultural norm is considered disordered. Please also review AIHCP’s Healthcare Certifications
Personality in itself is an essential feature to a person. It involves a person’s overall demeanor, it includes how a person reacts internally and externally with others and the person’s overall temperament. Overall, a personality is one’s unique patterns of thinking, acting and feeling (Myers, 2019). There are numerous theories of personality ranging from the psycho-analytic schools to the humanistic as well as the behavioral schools of psychotherapy. All emphasize their targeted areas of study to the development of personality and all add unique elements to understanding personality. Within personality, exist various traits that are essential to proper functioning within the norms of society. Traits are characteristics or behaviors or dispositions of how a person feels or acts in certain ways (Myers, 2019). Experts list the Big Five Factors of traits that determine personality factors. Myers lists Conscientiousness, Agreeableness, Neuroticism, Openness and Extraversion (2019). When one sways from one extreme to the other in these traits, then imbalance occurs. In addition, the DSM-V-TR also lists these traits in its alternate diagnosis for personality disorder with openness being replaced with lucidity (2022).
When an individual deviates from the cultural norms of his or her culture and society and these extremes manifest against the core basic traits, one will witness odd or deviated social behavior, but isolated acts of misconduct or erratic behavior do not constitute a disorder. A disorder is far more deeper and its duration long lasting. In this blog, we will take a closer look at personality disorders and their striking deviations from cultural norms and behavior.
The DSM-V-TR points out that an enduring pattern of inner experience and behavior that deviates from expectations of one’s culture constitutes a personality disorder. These disorders manifest in one or two ways, via cognition, affectivity, interpersonal functioning or impulse control. The DSM-V-TR continues that these enduring patterns are inflexible and pervasive across the range of the person’s personal and social situations and interactions with others (2022). The DSM-V-TR states that these behaviors cause significant distress and impairment in social and personal relationships and this pattern remains stable and of long duration with origins in adolescence and early adulthood (2022). Obviously, these issues are not related to substance abuse, medication, or other mental defects.
The DSM-V-TR looks at moderate to severe impairment in traits to affect identity, self-direction, empathy and intimacy. In addition, these disorders can portray various distortions of personality traits to the extreme. They can manifest negative affectivity versus emotional stability, detachment versus extraversion, antagonism versus agreeableness, disinhibition versus conscientiousness, and psychoticism versus lucidity (2022). It is because of this one can witness in personality disorders a wide range of odd, eccentric, emotional, impulsive, egocentric, aggressive, violent, unempathetic, and manipulative traits.
The DSM-V-TR groups personality disorders into three clusters. Cluster A includes paranoid disorders such as paranoid, schizoid and schizotypal. Cluster B includes personality disorders such as anti-social (sociopathy/psychopathy), borderline personality disorder, histrionic, and narcissistic disorders. Finally, Cluster C includes avoidant personality disorders such as avoidant, dependent and obsessive compulsive personality disorders (not to be confused the OCD itself). (2022).
Of particular note, based on different case studies and surveys, the percentage of personality disorders within the general population is 9 to 10 percent suffering from some type of personality disorder in some degree or level (Barlow, et al. 2023). Ironically, many of the terms associated with these disorders, are used loosely in everyday vernacular towards individuals who may act a certain way in a given situation but not possess the disorder. Bad behavior, sin, vice, or whatever one wishes to label it is part of the human condition and people are not perfect. Personality Disorders are merely a persistent form of these behaviors at an extreme and rigid level. So, when diagnosing, anyone at some time or some point can see at least a couple undesirable traits and feel guilt or shame for exhibiting these actions. Ultimately guilt and shame and acknowledgement are key signs one does not possess the disorder itself.
Types of Disorders
Personality Disorders are divided into three clusters of paranoid, anti-social and avoidant
Paranoid
Paranoid personality disorders are in the realm of psychotic and the schizotypal form can sometimes be the premorbid phase of schizophrenia itself. One of the key elements is the disorder is persistent before and after any delusional of psychotic episodes.
Paranoid Personality Disorder constitutes a pervasive distrust and suspicion of others. Without evidence, they feel they are being exploited or harmed. They discover unfounded evidence of demeaning actions or threatening meanings in other individual’s remarks or cues. They are preoccupied with doubts of other’s loyalty to them and find it difficult to confide in others. They feel information can constantly be used against them. Emotionally, they can become angry and hold grudges due to the perceived threats (DSM-V-TR, 2022).
Schizoid Personality Disorder is a detachment from social relationships beyond intimate family. They also possess a restricted range of emotions. These traits continue before and after remission of possible psychotic episodes (DSM-V-TR, 2022). Schizotypal Personality Disorder is more severe and resembles Schizophrenia and other schizophrenic spectrums. It can also co-exist with them but also exists outside the psychotic psychotic episodes (2022).
Anti-Social
Anti-Social Personality Disorder is best known a pervasive and consistent pattern of disregard and violation of the rights of others, occurring since age 15 and must be at least 18 (DSM-V-TR, 2022). With diagnosis, three of the following traits must persist
failure to comply with social norms and laws
deceitfulness and pathological lying
impulsiveness and failure to plan
irritability and aggressiveness
recklessness and disregard for safety of self or others
consistent irresponsible behavior
lack of remorse or empathy
Anti-Social Personality lacks empathy and recognition of the rights of others
The DSM-V-TR continues in alternative diagnosis with emphasis on a distorted identity based on egocentrism and self-esteem deprived via power and gain and pleasure. Personal gratification is the primary goal and self direction absence of inhibitions that prevent those gratifications. There is a lack of emotional connection or empathy within the disordered person and intimacy and relationships are meant for exploitation or manipulation to meet one’s own needs. The DSM-V-TR in addition lists these traits of which 6 must be met
manipulation (antagonism)
callousness (antagonism)
deceitfulness (antagonism)
hostility (antagonism)
risk taking (disinhibition)
impulsivity (disinhibition)
irresponsibility (disinhibition)
Horrifying enough, there can be a psychotic specifier as well with psychopathic features which would constitute the differences between a sociopath and a psychopath. Depending on degree and opportunity, these individuals can be very dangerous in what they are willing or not willing to do to others. Many criminals possess these traits and those in trouble with the law. Many can understand something is wrong but fail to care or display empathy or guilt or emotion regarding their actions.
Narcissistic Personality Disorder is commonly comorbid with Anti-Social Personality Disorder. Narcissists, according to the DSM-V-TR, display a pattern of grandiosity. They require admiration and lack empathy. The disorder can manifest in early adulthood (2022). Five or more of the following are necessary for diagnosis.
grandiose self importance
fantasies of unlimited success, power and brilliance
believes oneself is special
requires admiration of others
sense of entitlement
interpersonally exploitative
lacks empathy
envious of others
severe arrogance
In regards to identity, they require excessive reference of others for self-definition. Deep down, they have lower self-esteems and without these appraisals, they can suffer emotionally. In addition, self direction is tied to gaining approval of others. Relationships and intimacy are more superficial as to the image it portrays. Empathetically, they are restricted in understanding the needs and emotions of others at the expense of their own (DSM-V-TR, 2022). Closely related is Histrionic Personality Disorder which faces excessive emotionality and seeking of attention (DSM-V-TR, 2022).
If the other anti-social disorders are more intellectual, then Border Line Personality Disorder (BPD) is the chaos of emotion. According to the DSM-V-TR, BPD is a pervasive pattern of instability in regards to relationships, self-image and affects which onsets in early adulthood (2022). Five or more attributes must be present.
frantic efforts to avoid real and imagined abandonment
pattern of unstable and intense interpersonal relationships
identity disturbance and unstable self-image
impulsivity with spending, sex, substance abuse, reckless driving or binge eating
recurrent suicidal behavior, gestures, threats or self mutilation
affective instability due to marked reactivity
chronic emptiness
inappropriate anger or controlling anger
transient stress related paranoid ideation
In regards to identity, BPD is marked by poorly developed and unstable self-image. Self direction consists of instability with goals and plans. Empathetically, individuals have a difficult time recognizing the feelings and needs of others. In regards to intimacy and relationships, there is a consistent intense, unstable and constant conflict with others (DSM-V-TR, 2022). They experience intense emotional lability, anxiousness, separation insecurity, depression, impulsiveness, risks and hostility (DSM-V-TR, 2022).
Avoidant
Avoidant disorders
Avoidant personality disorders include Avoidant Personality Disorder, Dependent Personality Disorder and Obsessive Compulsive Personality Disorder.
Avoidant Personality Disorder involves more than an introvert life style or bouts with anxiety but a pervasive pattern of social inhibition, inadequacy, and hypersensitivity to negative evaluations of self (DSM-V-TR, 2022). Four or more of the following are need in diagnosis.
avoids occupational activities
unwilling to get involved with others unless certain of being liked
restraint with intimiate relationships
preoccupied with fear of rejection
feelings of inadequacy
views oneself as unappealing, inferior or inept
avoids risks of engagement or new activities
Avoidant personalities are associated with low self esteem identity wise. Their self direction is distorted due to reluctance to pursue goals. Their empathy for others is distracted by their own internal fears and their intimacy is restricted due to shame and fear of rejection. Their traits include anxiousness, withdrawal, anhedonia and intimacy avoidance (DSM-V-TR, 2022).
Dependent Personality Disorder involves a pervasive or excessive need to be taken care of by others which leads to submission and clinging behaviors marked by separation anxiety which manifests in early adulthood (DSM-V-TR, 2022). Five or more of the following symptoms are required for diagnosis.
difficulty making everyday decisions without excessive advice and reassurance
needs other to assume responsibility in life
difficulty expressing disagreement
difficulty initiating projects
goes to excessive lengths for reassurance
feels helpless when alone
seeks relationships for security
fearful of abandonment
Finally, Obsessive Compulsive Personality Disorder concludes the avoidant disorders. This disorder is not to be confused with OCD which can be comorbid but unlike OCD which reacts to stressors and anxiety, OCPD exists in all situational relationships. According to the DSM-V-TR, it is represented by a pervasive pattern of preoccupation with order, perfection and mental and interpersonal control at the expense of flexibility which begins in early adulthood (2022). Four or more of the following symptoms are necessary for diagnosis
preoccupation with details, rules, lists, order, schedules, organization
perfectionism derails task completion
focused on work before any types of leisure
overconscientious, scrupulous and inflexible in matters of morals, ethics or values (not when accounted to religious or cultural identification)
unable to discard worthless objects
reluctant to delegate tasks to others
adopts miserly spending habits
rigid and stubborn
Those with OCPD compose their identity as correlated with work or productivity. Their self direction is complicated due to rigidity in completing tasks and meeting standards. They lack difficulty in empathy to understand the feelings and standards of others. Finally, their intimacy is restricted in relationships since they put relationships secondary to work and maintain a rigid and stubborn life with others (DSM-V-TR, 2022). They adhere to rigid perfectionism, perseveration in tasks, intimacy avoidance, and possess restricted affectivity (DSM-V-TR, 2022).
Etiology and Treatment
Personality disorders are both a product of nature and nurture with roughly 10 percent of the population suffering from them
Personality Disorders like all mental pathologies cannot be originated from one aspect of life but is a culmination of biological, genetic, psychological, behavioral and social factors. In addition, many possess comorbid mood disorders or maladaptive coping strategies involving substances. In the cases of Anti-Social Personality, it is obvious that there are genetic dispositions as well as biological deformities within the brain that restrict empathy and impulsivity (Barlow, et al., 2023). In addition, early childhood mistreatment, abuse, trauma, poverty and malnutrition can play roles in the development of life views and emotional affectivity (McRay, 2016). None of these things guarantee a disorder, but they collectively can contribute to disorders that later develop in early adulthood.
In children, values and morality are also essential to enforce in life. In early development of a children, egocentrism is important to survival but children are exposed to empathy, love and the needs of others. Children that are not properly guided can develop vices that later can lead to habitual life styles (McRay, 2016). Children with natural inclinations to pride, or selfishness, or other vices, without the proper guidance can fall victim to these inclinations as adolescence continues. These maladaptive behaviors manifest as the person is permitted without consequence to perform these actions. Obviously from a religious perspective, morality and restrictions are essential guardrails in anti-social personality development (McRay, 2016). Even without proper social norms and concepts such as the Golden Rule, individuals can develop into habitual disordered individuals in mind, thought, emotion and behavior.
Unfortunately, many individuals with personality disorders do not seek treatment. Avoidant groups are the most likely to seek help but anti-social and paranoid seek assistance less. Those who do find help require extensive and consistent counseling that focuses on emotional regulation, identifying distorted thinking, and understanding the needs of others. This involves comprehensive psychotherapy that includes CBT, DBT and other cognitive therapies. Humanistic therapies can attempt to at least encourage acknowledgement of the needs of others. Medication is rarely helpful but only to alleviate secondary symptoms of anxiety or depression, especially in BPD (Barlow, et al., 2023).
Pastoral and Christian Counseling care has existed well before modern psychology. In these practices, the proposed opposite virtue of the habitual vice was emphasized such as humility over pride or temperance over anger. In these cases, the spiritual treatment of the sinful condition was considered in addition to the mental pathology. Moral virtues, spiritual discipline, submission to God and constant regulation over viceful responses were considered critical. For many, faith left the change to the grace of God due to the sinful nature of humanity(McRay, 2016).Too many times, pastoral leaders or even counselors and mental healthcare professionals can become over involved in personality disorder cases looking to rescue and save these clients. Many of these clients unfortunately are sometimes beyond saving and will attempt to manipulate helpers.
In regards to loved ones, family is encouraged to never withdraw love but to always protect themselves from manipulation or abuse. In addition, they are to set strong boundaries with those facing personality disorders. Boundaries are essential and must be made clear and definitive of expectations but also demands for treatment. Family needs to become psycho-educated on the disorders and be able to identify manipulations or emotional states to better protect themselves but also help the person.
Conclusion
Please also review AIHCP’s Healthcare Certification Programs
Personality Disorders are habitual, persistent, and impairing traits that affect an individual’s ability to show empathy, regulate emotion, or interact with other people in a fair and just way. The disorders affect their ability to properly assert themselves in positive or negative ways. They manifest in types or paranoid, anti-social or avoidant. All individuals to some extent sometimes deviate from the norm or do something wrong, but personality disorders deviate from the cultural norm on a consistent basis and at disproportionate extreme. While those who suffer from these disorders, especially BPD and Sociopathy must be held accountable for bad actions, one still must understand the unnatural impulse that has habitually sidetracked their ability to operate as normal individuals. This leads to erratic, odd, distant, dysregulated, manipulative, rigid, emotional, or dangerous behaviors. These disorders have multiple origins from genetics, biology, as well as past trauma, and behavioral upbringing. It is difficult to predict what factors will lead to a true disorder but roughly 10 percent of the population suffers from a personality disorder. In regards to treatment, psychopathology and some medications can help alleviate anxiety and depression, but overall, a person must commit to life long therapy and continually identify their issues. Ironically, the inability to acknowledge this is the biggest issue for adjustment. Finally, it is important to form healthy boundaries with loved ones who suffer from these disorders. While many are hard to understand or even tolerate, it is important to remember they are broken. This does not mean one surrenders oneself to their desires, nor does it mean one justifies their actions or does not hold one accountable, but it does demand an empathetic condition for their brokenness.
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorder” DSM-5-TR (5th ed., text revision). American Psychiatric Association Publishing.
Barlow, D.H., Durand, V.M., & Hofmann, S.G. (2023). Psychopathology. An integrative approach to mental disorder (9th ed.). Cengage Learning
McRay, B.W., Yarhouse, M.A., Butman, R.E., & Kiple, C. (2016). Modern psychopathologies: A comprehensive Christian appraisal. (2nd, ed.) IVP Academic
Additional Resources
Personality Disorders. Cleveland Clinic. Access here
Burton, A. (2024). “The 10 Personality Disorders”. Psychology Today. Access here
Christian Counselors and Spiritual Directors help many individuals coming from deeper issues of loss, trauma, pain, and spiritual darkness that are searching for healing and love in the presence of God. The dichotomy of Christian theology that expresses the human soul as a child of God but at the same time notates the nothingness of self compared to God is a striking polar opposite. Obviously, a person in need cannot be declared as nothing and stripped of all goodness that innately exists within their personhood. With an awakening of self, the spiritual journey and crosses have life has injured many elements of self image and concept, so it is important to elevate self esteem but also eliminate pride. There lays the delicate balance of understanding and communicating the value of humility but also the praise of self in the healing process.
Humility ironically leads to greatness because it recognizes our dependency upon God
God the Creator, chose to create humanity from nothing due to His infinite love. As a creatures, it is an essential truth to acknowledge two things. First, creatures are nothing in comparison to the Creator and second, creatures owe the Creator everything. God does not wish to force servitude on His creatures, but He is the source of their creation and hence it is only natural and right that creatures worship and adore Him. This is not due to a sense of entitlement by God, or self-interest and pride in His greatness but a true reality of existence. When creatures cease to worship and serve the Creator, then their end becomes unnatural. This unnatural end results in corruption. Lucifer and his minions rejected this law of nature and instead chose their own will and attempted to alter the natural reality of existence by refusing worship and obedience to the Creator. The choice did not liberate them from worship but forever corrupted them in pain and suffering. Since God is infinite love, when one abandons self and seeks God, the act of worship is likened to breathing. It is natural and just.
As creatures, justice alone suffices to acknowledge the creature’s obligation to serve and worship. It also clearly points out the dependency and imperfections of the creature in relationship to the Creator. It would be a delusion of grandeur to glorify one’s stature, talents, appearance, or works as one’s own accomplishments without reflecting the design and influence of the Creator. This is not a false humility but a reality that every creature must accept as natural. When a creature attempts to glorify self, it leads to delusion and corruption, but when a creature understands its relation to the Creator, it lives in truth. Mary, the greatest and most magnificent creature ever created by God, teaches others one’s own nothingness. At the Annunciation. she responds to the Angel Gabriel’s salutation with a statement of her graceful state as a reflection of God and not of her own doing.
As Children
God transformed creation with His infinite love. He transformed creatures to His children, from something to someone and ultimately nothing to everything. God’s love elevates His creatures to children of God. It is in that relationship that individuals have true identity, self-image, value, and beauty. God created humanity in His own image and likeness according to Genesis. In this way, He infused intellect and will. This permitted His creation to possess a true image of the Divine that possessed sentience and freedom of choice. It permitted the relationship to be a mutual relationship of love as between parent and child. In this way, humanity became a prized possession of God, so much, that even after its fall, He was willing to become human, suffer, die and rise to save them from their own folly. It is through this additional act of love, beyond creation, but also redemption and sanctification that one sees the great value of one single human soul. The ransom price for each soul at the cross was a heavy price and God gladly paid it through Jesus Christ.
From this, one can see a balance of creature and child. Nothing and everything. It is within reflection and acknowledged dependence of the Divine that humanity’s nothingness becomes everything and it is through that a true Christian self esteem can emerge in a directee and spiritual child. It involves anchoring self-esteem and self-image to the connection with the Divine.
Christian Humility
Since pride corrupts and distorts reality between creature and Creator, then it is important to flee it and foster humility. Ironically, Scripture points out, the last will become first, and the one who destroys his own life will save it. These phrases in Christianity all point to a deeper mystery. It points to the truth that for one to truly find value in self, it is dependent upon complete rejection of self. This is clearly the opposite message of Lucifer and his fallen temporal world. The world whispers success at all costs, elevation of self, collection of riches, and exaltation of achievements. In modern psychology, congruence is seen as self-fulfillment and finding happiness in what one deems to be good. So many false images of happiness are sought to fulfill one’s own ego and desire in the mirage of temporal happiness only to be illusions that lead to chaos, loss, dissatisfaction, and moral degeneration. As Lucifer looked to idolize self, and how Adam sought self actualization without God, the temporal and secular man seeks self approval, pleasure and acknowledgement of others. The demand and adoration of the narcissistic self distorts the reality of creature and attempts to worship self as Creator. While this may seem subtle and maybe not as dramatic as Lucifer or Adam, the continuation of actions and their temporal gratification and glorification of self create narcissistic qualities that through habit become one’s own deification. Whether its through social media, fame and fortune or power, the creature becomes intoxicated with self and loses its identity. This in turn leads to corruption as pride, the source of all sin, leads to further deformity in greed, avarice, lust and envy for more. It is of no wonder then that creatures then attempt to define their own laws of moral conduct since they have become their own god.
Christian humility is the answer to this disastrous corruption of self. It is not a degradation of self but is a truthful mirror of a creature in dependence of a Creator. Like new born babies and infants, Christian humility acknowledges the need of a parent and the inability to exist or succeed without the Divine. It acknowledges that all accomplishments, successes, fortunes, riches, blessings, talents, virtues, and spiritual progress are God’s grace. It acknowledges that the creature cannot walk without the gentle guidance of the Creator. Likening the fallen world to a baby’s crib or playground, the great empires that are built in the creature’s mind are merely tall Lego blocks as compared to omnipotent and eternal presence of God. To exalt such feeble success to infinite greatness is a folly that Christian humility illuminates. Christian humility in spiritual direction does not look to tear the person’s success down, or make the person feel insignificant, it seeks to awaken the person from the illusion of the Matrix and to embrace the truth that all good comes from God and not self. Humility protects the creature from corruption and aligns the creature to reality and truth so that it can grow and become fulfilled as a child of God. Humility teaches a far greater self value then the self can ever afford for it is supported by a Divine enterprise and loving Father.
When the God, via the Second Person, became incarnated in Jesus Christ, He taught creation these truths. Jesus highlighted the folly of self adoration and the foolishness of seeking the world before the soul. Jesus refused the powers afforded to Him by a mere creature, namely Lucifer. Who in his delusions sought as a creature to afford the Creator power and wealth in a fallen world. Jesus rejected the pride of Lucifer in the desert and revealed the truth that humility over pride is reality. Jesus did not grant Himself a rich palace, but instead chose to be born in a stable. He lived for 30 years under moderate means as a carpenter supporting His mother. He enjoyed life in its simplicity as a testament to truth of reality. In His ultimate act of humility, as both God and man, the omnipotent and eternal God, hid Himself in His humanity and permitted the profane hands of creatures to mock and crucify Him. He stood before the pompus pride of Pilate and permitted this execution to take place, although as Creator, He could at any moment smite the entire Roman legion. In this humility, He surrendered Himself willing out of love for all His creation to be openly executed. He never reprimanded them, or exposed His Creatorship but with humility accepted the will of the Father. Christ said to His apostles regarding this fallen world, that if this place rejected Himself, the Creator, it will reject His followers. He taught them to seek these injustices, these rebukes, and embarrassments and to offer them to God. These slights should be seen as opportunities to suffer with Jesus and for Him to offer our imperfect deeds to the Father in His name.
In the text, “The Spiritual Combat” by Dom Scupoli, like many writers of his time, there was a great emphasis to acknowledge the nothingness of self. One sees this in the writings of Avila, as well as Loyola. Scupoli states that one should completely distrust self and place all trust in the Creator. In doing so, one accepts the reality that without God, one is truly nothing. One cannot do a single good deed without the merits of grace earned for oneself by Jesus Christ. In addition, one should honestly realize that without the gift of love from God, one deserves nothing from God, but nonetheless owes Him everything. Scupoli points out that pride corrupts the soul and breaks one from the reality of a creature’s true status. One should then seek the opportunity to be humbled by others and to always reflect one’s accomplishments to God. In this way, one experiences the truth of reality and avoids the destruction of self glorification.
Self Esteem in Counseling Vs Christian Humility
Christian humility acknowledges God as Creator and source of all our gifts and virtues. Please also review AIHCP’s Christian Counseling Certification and Spiritual Direction Program
While many humanistic counselors may see the degradation of self and one’s inability to do good without the external source of God as undignified, the reality is it prevents the disastrous lies that lead to vice and ultimate maladaptive coping. Self-esteem is critical for the depressed and broken. Individuals need to be taught to respect themselves, to love themselves, and to find joy in success. Counselors help them cultivate the tools to create and meet goals. It is healthy to find “pride” in accomplishments. It is also not sinful to accumulate temporal goods and find joy in temporal successes. However, when the source of one’s self esteem is rooted in self-glorification and one’s own morality and laws, then it becomes untruthful to reality and can cause degradation and misery. One’s self-esteem must be tied to God. When tied to God, it is more than it can ever be alone. One whose self-esteem is tied to God values and loves oneself because God loved oneself first. One whose self-esteem is tied to God is placed on an objective and unbreakable foundation of Divinity rather than shaky subjective weak foundation of frail humanity. Finally, humility with God grants a calm sense of peace in the presence. Unlike pride which is always moving and self serving, seeking and never content, humility grants peace about the past and security about the future. Depression of the past or anxiety of the future is tied to pride and not humility. The humble soul is content and secure in the grace of God because it submits to His will and serves Him.
It is natural than that true self-esteem correlates not with humanistic pride and narcissism, but with Christian humility. The acknowledgement of weakness and dependency does not weaken self-esteem, but grants it the source of its power through the Creator. Humility grants to the Creator His reflection and image in the creature. This humility then elevates the creature beyond any limits imaginable. This may not translate in this valley of tears as success but it does translate in eternity with Christ by emulating Christ on earth. Christ’s message of truth was humility because it frees oneself from the illusions of Lucifer. A great saint once said, the greatest weapon against the devil is humility because he does not know it.
Humility and Psychology
Since humility is so critical to salvation, it is no wonder then that is critical to temporal existence as well. While counselors help navigate individuals through issues of depression and low self-esteem there needs to remain a balance that does not transgress into narcissistic behavior. While even secular psychology looks to free the self to find happiness, even it recognizes the dangers of extremes in behavior. When self esteem becomes narcissistic pride it becomes dysfunctional and socially impedes a person’s mental and emotional progress in life. In the article, “What Is Humility & Why Is It Important?, Schaffner points out various critical elements of humility in psychology and social interaction. She points out that humility is key accurate self portrayal, modesty and awareness of others (2020). In addition, Schaffner lists other key elements of humility which include a willingness to see one’s true self, an understanding of one’s appropriate place in the world, an understanding of one’s faults, limitations and mistakes, a true openness to change, a focus on others, and an ability to appreciate other things outside ourselves (2020).
Like the spiritual benefits, the emotional and psychological benefits seem to both open oneself to others, service, and truth. Pride that becomes malignant is detrimental to self, growth and society. Pride becomes an injustice to reality, self and others. It makes sense than that a Christian perspective on humility is far from detrimental to self-esteem but in reality beneficial.
The Devil and Spiritual Pride
Pride becomes narcissism and creates the illusion of greatness which leads to corruption.
For those who seek God, spirituality opens many doors of illumination and unity with Him. However, like the souls who seek power in secular venues, spiritual people can befall pride in spiritual endeavors. Instead of riches and money and fame, the soul boasts of virtue and sanctity and holiness. Scupoli notes that this is one of the traps of the devil. Individuals exposed to the world are ensnared differently than individuals seeking spiritual perfection. Like the Pharisees, spiritual virtue becomes source of power over others. It becomes their own cultivating gifts instead of a grace given by the Creator. These souls then find pleasure in their own virtue as a end in itself. In this pride begins to rot within the soul. Instead of thanksgiving, gratefulness and humility for grace, the individual gravitates towards holy deeds as their own. In turn, instead of empathy for others in sin, they find judgement. Instead of reflection of their own failures and past falls, they only condemn those committing the same offenses. They feel a sense of entitlement and status and wish for their spiritual sanctity or message to be seen and heard. They fall into disobedience to spiritual authority and envy others of spiritual status, as well as seek ways to overcome spiritual rivals. This is the corruption instilled by Satan in spiritual pride. It utilizes the same schema but unlike utilization in a secular setting, it finds its use in a spiritual one. This is why Christ was so abrupt with the Pharisees because He understood their rottenness and pride.
Scupoli recommends that individuals flee all vanity in the spiritual life and to recall one’s own distrust of self and complete reliance of God. While thankful and happy to receive graces from God as any child, he also reminds one to never believe that these gifts are a result of sanctity or worthiness. He warns one to never find disgust in another’s faults but to remember the same faults that exist in oneself and if not for God’s grace, how one would be no better. He reminds one that one fails God or sins to not scrupulously over analyze the fall but to seek immediate forgiveness. When one over analyzes failure, one tends to oppositely attribute success or failure as to one’s own means. One can never reach perfection. One is never worthy. Only through blood of Christ and the ransom paid is one made worthy. A humble soul participates with Christ but no works or deeds can ever save himself but only through the faith of Christ which produces a living faith of works energized by His grace. So, no matter how hard one may try to reach Christian perfection, no creature of himself or herself can ever be perfect. Many sincere souls rightfully fear offending God and seek each day to avoid sin at all costs. While this is important, it is equally important to understand that one when fails, it is due to our one’s own brokenness and one cannot allow pride to seep in the crevices of thinking one cannot sin. Humility since it is based in truth is also aware of brokenness and sin as a part of an imperfect nature due to Original Sin. Hence when sin occurs, one should humbly acknowledge the brokenness and pray harder to God for future graces. Humility constantly re-directs oneself to God after sin because it acknowledges that oneself cannot live a good life without God’s grace.
Scupoli reminds individuals that sin and suffering and crosses are tools God utilizes to foster humility. Through failures, the soul realizes even more so its utter dependence upon God. The moment the soul falsely feels it can move forward of its own devices and virtue, then it is destined for failure via the vice of pride. In this way, God reminds His children that they need Him, not out of arrogance but out of necessity of reality.
Conclusion
Work hard, stay humble and reflect all greatness to God in your life. Please also review AIHCP’s Christian Counseling Certification and also its Spiritual Direction Program
Christian humility is not meant to deface self-esteem, or identity. It is meant to strengthen it through connection with God. It is based in reality and not the false assumptions and illusions of the world that celebrate arrogance, power, and success over piety, reliance and thanksgiving. Pride is the great illusion of self where one puts self on a pedestal as god. It corrupts and destroys like it did to Lucifer. The great deceiver hopes to trick humanity into being prideful about self and elevating the creature to the level of Creator. It is not depraving or neglectful to rightfully and truthfully understand one’s nature of dependence upon God. It does not depress self-esteem but permits self-esteem to actualize itself through the connection of grace with God. Humility is the tool for this relationship because it, unlike pride, acknowledges the reality between Creator and creation.
Mood disorders transcend the usual care of pastoral or non-clinical grief counselors. Most grief counselors deal with the natural phenomena of loss that follows a natural grief trajectory. Clinical professionals, who may also be grief counseling certified, deal with pathological issues surrounding mood. Any instability of extremes, whether due to mania or melancholy can disrupt natural life and harm mental health. Sometimes, moods can be directly affected by an acute grief or loss and this leads down a trajectory of complications due to grief, while in other cases, there is no triggering loss that causes the pathological mood. Instead it involves an in-depth investigation into the etiology of the disorder reviewing biological, genetic, psychological, social and spiritual issues to explain the condition.
The DSM-V-TR lists numerous mood disorders ranging from Major Depressive Disorder to Bi-Polar Disorders. Please also review AIHCP’s Grief Counseling Certification
The DSM-V-TR groups together a variety of mood disorders which in this blog will highlight Major Depressive Disorder, Persistent Depressive Disorder and its numerous specifiers, as well as Bi-Polar 1 and Bi Polar 2 disorders and finally, Prolonged Grief Disorder. It is important to remember that for the pastoral or non-clinical grief counselor, one should have a strong understanding of these mood disorders to help refer clients to the appropriate clinical specialists. A non-clinical grief counselor cannot diagnose or treat mood disorders but they can be trained to spot these disorders and work with clinical professionals in assuring the necessary therapy and medications are received for the client.
Mood disorders find their etiology from numerous factors. Biologically, whether mania or melancholic, there is a strong connection of genetic inheritance of these pathologies tied to the neurotransmitters (McRay,2016). When the neurotransmitter, serotonin, is low, depressive states can exist. Serotonin is the a critically important neurotransmitter for mood stability (Barlow, et. al., 2023). In regards to mania, the synapses between neurons fire to fast, and a euphoric state overtakes the person. This is usually due to higher levels of the neurotransmitter norepinephrine and lower of levels of serotonin, although higher levels of serotonin can also lead to states of mania (McRay, 2016).
Depression can be caused by an internal trigger but also a stressor or external loss. Hence unipolar mood disorders can be both have a direct external stimuli as well as an internal disruption. Many times the diathesis or culmination of internal and external events that overcomes a person to the disorder can be attributed to external factors that activate it. As similar to anxiety disorders, a loss, or lack of social support in that loss, or distorted cognitive thinking can unravel a person’s natural reactions into a pathological state (Barlow, et. al. 2023).
When considering psychological etiology for mood disorders, many aspects involve self image, cognitive distortions, as well as learned helplessness in situations. When individuals engage in self negative talk and think the worst, then it can affect a person’s overall mental paradigm. In addition, when a person feels they have no control or power to prevent bad things from continuing, then the person becomes susceptible to pathological mood disorders (McRay, 2016). In addition to how one thinks, social and cultural and spiritual aspects play a key role. A person’s support system is key in any mood stabilization because it determines the foundation one has to face multiple problems before succumbing to the issue. In addition, culturally and spiritually, how one views loss can play a key role in how one reacts to loss.
As one can see, mood disorders are a complications of genetic but also psychological, social, cultural and spiritual aspects of the person. Sometimes, the mood disorder, such as depression, has a visible trigger, but other times, it is purely at the chemical level of the brain. Every individual is different and what causes diathesis and activation of a mood disorder, or even anxiety is not a simple equation but a very complex one.
Mood Disorders and the DSM-V-TR
In this blog, we will follow the order of the DSM-V-TR and how it lists and discusses the nature of mood disorders. We will primarily focus only on the above mentioned disorders.
Bi Polar I & Bi Polar II Disorder
Polarity of symptoms Depression euthymia mania subsyndromal hypomania. Vector illustration
Bi polar disorders are characterized by cycles of depression and euphoria (mania) with symptoms that can greatly affect one’s ability to function in life (McRay, 2016). The DSM-V-TR states that mania is a period of abnormal and persistent moods of high levels of energy with the possibility of also irritability which lasts at least 1 week (2022). During this phase of mania, the DSM-V-TR notes these types of characteristics with three needed for diagnosis or four if the mood is only irritability.
inflated self esteem or grandiosity
deceased need for sleep
more talkative or need to talk
flights of ideas or subjective experiences that are racing through the mind
distractibility
increased goal directive activities that can be social, work, academic or sexually
excessive engagement in activities with high potential for bad outcomes. Such as foolish business investments, spending sprees or sexual activitiy
The DSM-V-TR continues that these states cause severe impairment to social and occupational functioning and has no association with other psychotic, psychological, substance or medicated purposes (2022). Within itself, these are conditions for mania, which albeit rare, can exist as an issue alone apart from Bi-Polar I or II.
Ironically, Bi-Polar I does not require a depressive cycle although that is very rare for one not to be present in diagnosis. When we discuss Major Depressive Disorder and a depressive episode we will list its diagnosis as well which would be utilized with any Bi-Polar disorder.
For Bi-Polar I, as well as Bi-Polar II, the DSM-V-TR provides many specifiers since it affects individuals with so many additional subjective aspects. It can be mild, moderate, severe, possess psychotic features, be in partial remission or full remission, or also include anxious distress, mixed features, rapid cycling, melancholic features, mood congruent psychotic features or mood incongruent psychotic features, catonia, peripartum or seasonal (2022).
Bi-Polar II differs from Bi- Polar I in that there is no state of mania but there always must be a depressive state. What replaces mania is referred to hypomania. Hypomanic episodes shares the same characteristics of mania but not as severe or impairing to the individual (only 4 days as opposed to at least a week) but it still manifests a change in functioning that is not characteristic of the individual when not symptomatic (2022). In addition, the mood shift is observable by others but not enough to cause extreme distress (DSM-V-TR, 2022).
The primary differing diagnosis factor from Bi-Polar I over Bi-polar II is one has not ever been diagnosed with a true mania state ever in life.
It is important to note, some individuals who suffer from Bi-Polar mood disorders cycle more rapidly than others, with 4 mood shifts a year being considered high but there can be less cycles and individuals can move through them quickly (Barlow, et. al, 2023).
Major Depressive Disorder
While depressive episodes are part of bipolar disorders, the same criteria for Major Depressive Disorder that diagnoses an episode of depression for Bi-Polar disorders is also diagnosis Major Depressive Disorder but without any mania or states of euphoria. Major Depressive Order can find its origins biologically or also be a reaction to a loss or severe stressor. It is a unipolar mood disorder without a switching from extremes but a state of melachony
Facing Major Depressive Disorder
According to the DSM-V-TR depressed moods or loss of interest in pleasure must persist for periods of 2 weeks or longer (2022). Diagnostic characteristics include the following and requires five or more symptoms for diagnosis.
Depressed mood for most of the day or nearly everyday. Feelings of sadness, emptiness and hopelessness
Diminished interest in pleasure
significant weight loss
Insomnia or hypersomnia nearly or everyday
psychomotor agitation that is observable by others
fatigue and lack of energy nearly everyday
feelings of guilt or unworthiness
diminished ability to concentrate or think or make decisions
recurrent thoughts about death, recurrent suicidal ideation without a specific plan or with a plan, as well as suicide attempt
These symptoms impair the individual in all aspects of life and are not due to any other psychological, medical or use of substance (2022).
Like bi-polar mood disorders, Major Depressive Disorder also has specifiers that dictate mild, moderate, severe, with psychotic features, partial or full remission, with anxious distress, mixed features, melancholic features, atypical features, mood congruent or mood incongruent psychotic features, catonia, post partem, or seasonal patterns (SAD) (DSM-V-TR, 2022).
Overall, Major Depressive Disorder is one of the most common mental maladies. It is considered the common cold of mental health (McRay, 2016). Women are 2 to 1 more likely to develop it, while Bi-Polar Disorder is equal (McRay, 2016).
Mentally, an individual suffering from depression faces the depressive cognitive triad that perceives negative connotations about self, the world and the future (Barlow, et. al., 2023).
Persistent Depressive Disorder
Persistent Depressive Disorder differs from Major Depressive Disorder in that is lasts longer than the normal minimum of 2 weeks but untreated can persist for months to years to decades. It is not as intense but it leads to numerous health and mental issues. Diagnosis requires a consistent 2 year period. It includes poor appetite or overeating, insomnia or hyperinsomnia, low energy, low self-esteem, poor concentration and feelings of hopelessness, (DSM-V-TR, 20220). Individuals can also suffer from both Persistent and Major Depressive.
Other Mood Disorders
Other mood disorders include Disruptive Mood Dysregulation Disorders that deal with frustration and anger outbursts, as well as Cyclothymic Disorder which does not meet criteria for mania, hypnomania or depressive episodes but still possess similar traits at a less severe level but for a period of 2 years with impaiment.
Ironically, Prolonged Grief Disorder is not associated with mood disorders in the DSM-V-TR but is a stress related disorder to acute grief which resembles depression but is a complex grief reaction. The trajectory of normal reaction to loss is distorted due to severity of the loss, or various subjective factors involving the person. AIHCP has numerous blogs on Complicated Grief as well as Prolonged Grief Disorder.
Treatments for Mood Disorders
Treatment for mood disorders should also include a integrated approach that includes medication as well as therapy. Medication only masks the problem and without life skills and abilities to understand distorted thinking, then long term healing and mental health is not possible. Also, some medications have complications which involves alternate trials and errors of different medications. In addition, many individuals feel a mental stigma when diagnosed with depression or bipolar disorders. This leads to hiding these feelings, or refusing to take the appropriate medications. This leads to continued chaos, impairment, broken relationships, loss careers, and wasted time. It is important to face mood disorders as any health condition.
SSRI help stabilize serotonin and mood
Medications
Anti-depressants are utilized to help most individuals with mood disorders, especially melancholy. There are three types. First, SSRIs are the most common and most used in modern medicine. Second, tricyclic and third, monamine oxidase (MAO). The tricyclics are rarely used with the advent of SSRI’s since tricyclics had more side effects. SSRI’s stand for Selective Serotonin Reuptake Inhibitor. They prevent the transfer of serotonin from one neuron to another hence preserving a higher level of serotonin to the body to help maintain mood. MAO’s help dissolve the break down of Serotonin (Barlow, et. al., 2023). Barlow notates that 60 to 70 percent of individuals who take medication for depression experience improvement, with half of that meeting full to close recovery to full functioning (2023). A common SSRI’s include Prozac (fluoxetine). Others include Celexa, Lexapro, Luvox, Paxil and Zoloft. Sometimes, individuals must go through a regiment of different SSRI until they find the best fit and dosage necessary to manage the depression. Some need to be on SSRI longer, while others are dosed and gradually let off as needed.
Those who face treatment resistant depression can also turn to other methods to treat depression. Holistic and natural remedies under the guidance of a primary physician such as St. John’s Wort or hypericum have shown benefits as well (Barlow, et. al., 2023). Other more direct methods include Transcranial Magnetic Therapy (TMT) as well as Electroconvulsive Therapy (ECT) which directly sends impulses into the brain and neurons (Barlow, et al., 2023).
In regards to bi-polar disorders, a lithium based medication is utilized to help with mania. Lithium, a common salt in the natural environment, needs to be carefully dosed but has success with controlling mania states. It is associated with weight gain which is another reason many individuals with bi-polar disorders wish to avoid their medication (Barlow, et. al., 2023).
Psychotherapy
Psychotherapy when supplemented with medication is the best combo for treating mood disorders. It is important to fix the chemical issue but one also needs to have a strong understanding of self and ways to think differently. Cognitive Behavioral Therapy plays a key role in helping individuals reframe and rethink distortions and negative connotations about self. An individual who is depressed already has negative connotations about self, the world and the future. AIHCP has blogs about CBT and its importance as a behaviorist therapy stemming from Aaron Beck and Albert Ellis that looks to help individuals think more healthy for better behavior and mental functioning. In addition, human centered therapies which gravitate towards self esteem and congruence and fulfillment are important. Karl Rogers and his person-centered therapy looks to support the client in meeting fulfillment through empathy, genuineness and unconditional positive regard. AIHCP also has a blog to review on human-centered therapies. Finally, interpersonal skills and support is key. Individuals suffering from loss need support. An individual with better support systems can overcome different losses with more success. Some have stronger internal systems of meaning and spirituality, while others may have more family or friends or financial means to overcome loss. Basic grief counseling in these ways can help individuals become more resilient when depressed or sad.
Conclusion
Please also review AIHCP’s Grief Counseling Program
Mood disorders can be stable with only one extreme or unstable and shift from mania to melancholy. They are among, with anxiety, the most common psychopathologies. Unfortunately, many individuals avoid treatment due to social stigma. It is important to find the time to take care of one’s mental health if afflicted with a mood disorder. Mood disorders can be genetic or causal but most all have solutions via medication, psychotherapy and counseling, or an integrated approach.
Please also review AIHCP’s Grief Counseling Certification as well as AIHCP’s multiple other behavioral health certification programs.
Clinical Depression (Major Depressive Disorder). (2026). Cleveland Clinic. Access here
Dimaria, L. (2026). “Types of Mood Disorders”. VeryWellMind. Access here
References
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorder” DSM-5-TR (5th ed., text revision). American Psychiatric Association Publishing.
Barlow, D.H., Durand, V.M., & Hofmann, S.G. (2023). Psychopathology. An integrative approach to mental disorder (9th ed.). Cengage Learning
McRay, B.W., Yarhouse, M.A., Butman, R.E., & Kiple, C. (2016). Modern psychopathologies: A comprehensive Christian appraisal. (2nd, ed.) IVP Academic
Researchers have studied the Dark Triad of psychopathology since 2002. This group includes psychopathy, narcissism, and Machiavellianism. The topic has gained much notice in academic circles and public talks. Many peer-reviewed articles show this growth. These papers explain and examine the complex parts of these linked personality traits. Early research showed how these traits overlap. A shared core of cold manipulation defines them. Scholars now see that each trait has many sides. This view challenges older ideas that viewed each trait to be one unit. Studies on the Dark Triad now include talks about measurement differences and method concerns. These include using easy-to-reach samples and relying on single ways to collect data. We must fix these issues to help our understanding grow. Doing so will make future studies in this field of psychology stronger.(Joshua D Miller et al., 2019). While initial research underscored their conceptual overlap—characterized by a shared core of callous manipulation—scholars have increasingly recognized the multidimensionality of each trait, challenging earlier perspectives that treated them as unidimensional (Furnham A et al., 2013). Consequently, the landscape of Dark Triad research has evolved to include discussions on measurement discrepancies and methodological concerns, such as convenience sampling and the reliance on mono-method approaches. Addressing these issues is crucial for advancing our understanding and ensuring the robustness of future studies in this significant area of psychological inquiry.
The Dark Triad. Please also review AIHCP’s Healthcare Certifications
The Dark Triad includes Machiavellianism, narcissism, and subclinical psychopathy. These three traits form a group of harmful personality types that psychologists study often. These traits share a core of cold and manipulative behavior. This behavior often causes harmful results in social settings and interpersonal relationships. Recent studies show how these traits overlap and how they differ. They are key tools for understanding complex human actions in the study of mental illness. Researchers look at where these traits start and how they appear in people. This work shows how the traits lead to antisocial acts and damaged relationships. New studies on dark personality traits show why they matter to abnormal psychology. This base of knowledge calls for more study on how these traits affect mental health and how society works.(Furnham A et al., 2013). Furthermore, explorations into the origins and manifestations of these traits underscore their significance in the development of antisocial behaviors and dysfunctional interpersonal relationships, a point emphasized by emerging studies on dark personality traits and their relevance to abnormal psychology (Thomaes S et al., 2017). This foundation invites further inquiry into their implications for mental health and societal functioning.
Importance of Studying Psychopathological Traits
Psychologists must understand psychopathological traits for research and practical use in various fields like clinical psychology, criminology, and organizational behavior. The Dark Triad includes Machiavellianism, narcissism, and psychopathy. It helps explain harmful social behaviors like manipulation, self-interest, and a lack of empathy. Researchers study these traits to see how they link to poor social behaviors and relationships. Scientists created short tools like the Short Dark Triad (SD3). These tools help test people in both clinical and general groups (). More Dark Triad studies appear. Psychologists place these traits into larger psychological models to see the structure of personality and what it means ().(Daniel N Jones et al., 2013)). Additionally, as the literature surrounding the Dark Triad expands, it becomes increasingly relevant to place these traits within broader psychological frameworks, enhancing our understanding of personality structure and its implications ((Furnham A et al., 2013)).
As science progresses, there are clear ties within the brain’s ability to foster emotion, regret, or remorse attached to the amygdala. Yet, one cannot simply justify such extreme and vile behaviors that fall under the category of anti-social disorders, simply because one does not feel. One can understand how it may be easier to be cold and ruthless, but one still possesses the knowledge of right and wrong. While secular science only studies the biological, many spiritual counselors believe there is more than just merely a physiological issue, but also a spiritual one. Vice, habitual immorality, moral relative attitudes, and evil influences can also contribute to an individual who displays such disregard for other human beings.
The danger becomes when there is no balance in understanding these individuals. If one looks for only empirical studies at neglect of spiritual, or if one dismisses the science for only spiritual answers, then the whole story will not be presented. It is important to understand both elements. So, counselor should be well versed in the scientific explanations and reasons why individuals do not feel or show empathy, but also beyond the biological, review the behavioral history, trauma, and other spiritual distresses that have allowed this malignant personality to fester. There will be differing degrees of where one falls, but also different levels of how far someone will go in regards to hurting another person.
Characteristics and Behavioral Patterns
The Dark Triad of Psychopathology includes Machiavellianism, narcissism, and psychopathy, and these behavioral patterns show a shared tendency to both manipulate and exploit other people in their lives. People with these traits often show a liking for lies and a clear lack of empathy. They chase their own interests in both social and work situations at all times. Research grew a lot after the framework began, showing different connections and how these traits work together in various settings [citeX]. The creation of reliable tools like the Short Dark Triad (SD3) shows the urgent need to test these traits well and quickly in many groups [extractedKnowledgeX]. We learn more about how these traits affect interpersonal relationships and societal dynamics by understanding these characteristics.(Furnham A et al., 2013). The development of reliable measurement tools, such as the Short Dark Triad (SD3), underscores the urgent need to assess these attributes efficiently and effectively in diverse populations (Daniel N Jones et al., 2013). By understanding these characteristics, we gain insight into their broader implications for interpersonal relationships and societal dynamics
These individuals will be very self-centered, proud and vain. They will exhibit charm and charisma for who they want but will ruthlessly remove (at varying levels) those who pose a threat to them. They will manipulate and see individuals as pawns to their own needs. In addition, some will be cold and calculating while others may be very emotional in outbursts. This varies pending on if they are a psychopath or sociopath. In addition, they hold to a strong subjective morality that values their belief system over others. In addition, they may be extremely greedy, lustful, or possess other vices at high levels.
While many of these anti-social behaviors at the biological level, or exist due to past trauma and abuse, one cannot easily dismiss the lack of virtue in their lives. At one point, one has to accept responsibility. While it may be difficult, one cannot live a sinful and vice filled life and justify it due to the past or biological factors. While these issues can contribute to their condition, these individuals still possess free will and can choose to better themselves.
While they are not as common, these individuals do exist. Unfortunately, many times, individuals hurl these names onto people they are upset with. A person can exhibit some traits, or vices in life and not be clinically diagnosed with any of the three personality disorders. All human beings can be selfish, or use others at times, but individuals who truly are clinically narcissistic, or psychopathic, behave habitually not randomly. They exhibit the behaviors universally and have zero ability to show remorse. Some are clinically worst than others. Some are far more dangerous than others in the lengths of their plans, but a person who truly exhibits these behaviors at a clinical level is unforgettable.
Psychological and Neurological Underpinnings
The psychological and neurological roots of the Dark Triad show how complex these antisocial traits are. The triad includes psychopathy, narcissism, and Machiavellianism. Research shows these traits share a harsh core of callous manipulation. This manipulation appears through clear behavior patterns and emotional reactions. For example, people with these traits often exploit others. They show a lack of empathy at the same time. This lack of empathy links to specific brain differences. One difference is lower activity in the amygdala during emotional processing. This lack of brain activity helps researchers understand the motives behind Dark Triad behaviors. Researchers look at how these traits work together using different models. New studies emphasize how these traits relate to broader mental health issues. Explaining these psychological and neurological models gives useful ideas about how these traits continue and spread. This work helps people understand abnormal psychology more clearly.(Thomaes S et al., 2017). Consequently, elucidating the psychological and neurological frameworks can provide significant insights into the maintenance and proliferation of these traits, contributing to a more comprehensive understanding of abnormal psychology (Furnham A et al., 2013).
Psychopathy
Psychopaths, as well as sociopaths have no remorse
Psychopathy is a major part of the Dark Triad of Psychopathology. It connects to narcissism and Machiavellianism but has unique features that set it apart. This personality trait shows a total lack of empathy and weak emotional reactions. It leads to a habit of manipulating others. Research finds psychopathy includes coldness and acting on whims. These traits put people at a higher risk for breaking social rules and acting against society. Recent meta-analytic findings show these dark traits are related. They are separate but have similar effects on behavior and personality structure. This is true for traits like agreeableness in the Big Five model. Experts put psychopathy in the interpersonal circumplex and Five- and Six-Factor models. This proves the trait has many parts and is hard to measure. Understanding psychopathy is needed to deal with its impact on society.(Muris P et al., 2017). Moreover, psychopathy has been situated within both the interpersonal circumplex and the Five- and Six-Factor models of personality, underscoring its multifaceted nature and the complexities of measuring its manifestations (Furnham A et al., 2013). Understanding psychopathy is essential for addressing its societal consequences effectively.
Sociopathy can also find itself within these conditions. Sociopathy and Psychopathy are similar in that neither express remorse or feel emotion but sociopathy is more a learned behavior as opposed to psychopathy which is genetic. Both represent issues within the brain to feel and express emotion, but there reactions also vary. Sociopaths tend to be more impulsive or reactive and emotional, while psychopaths are more calculating and controlled.
Narcissism
Self love and Narcissism
Narcissism is one trait in the Dark Triad of Psychopathology, and it affects interpersonal relationships and self-perception in a unique way. Narcissists show grandiosity and need constant admiration, but they lack empathy and value their self-image above all else. This focus causes great trouble in personal connections and leads to callous, manipulative behavior. Narcissists share these traits with Machiavellianism and psychopathy. Research shows narcissists may exploit others in an endless quest for validation and power. Narcissism connects with other Dark Triad traits, so we must study its impact more. This matters most in offices and social groups. In these settings, interpersonal actions change the results.(Furnham A et al., 2013). Research indicates that narcissists may engage in exploitative behaviors, driven by their insatiable quest for validation and dominance (Daniel N Jones et al., 2013). Moreover, the interplay of narcissism with the other traits in the Dark Triad underscores the necessity for further examination of its implications, particularly in social and organizational contexts where interpersonal dynamics significantly influence outcomes.
Core Traits and Manifestations
Studies on the Dark Triad show that Machiavellianism, narcissism, and psychopathy appear in different but connected ways. These core traits affect how people act and how they talk to others in their daily lives. Every trait shares a common base of coldness and manipulation. Paulhus and Williams described these features in their early work on the triad. These traits lead to harmful behaviors. They also play a large role in mental health disorders. We must understand how these complex traits work. The way these traits work together leads to many bad results. These results include fights between people and damage to mental health. Researchers study these traits more today. We must see how they fit into general psychology. This work helps experts find new ways to treat people who show these three traits.(Furnham A et al., 2013). These socially aversive traits not only contribute to maladaptive behaviors but also play a significant role in psychopathology, underscoring the need for a nuanced understanding of their complexity (Thomaes S et al., 2017). The interplay of these traits can lead to various detrimental outcomes, including interpersonal conflicts and detrimental effects on mental health. As researchers continue to investigate these traits, it becomes increasingly important to appreciate their implications for broader psychological frameworks, thereby paving the way for innovative approaches in the treatment of individuals exhibiting these characteristics.
Impact on Interpersonal Relationships
Machiavellianism, narcissism, and psychopathy make up the Dark Triad traits. These traits disrupt relationships and cause many negative results for both the people who have them and others around them. Research shows people who score high in these traits often use manipulation and exploitation. This behavior lowers trust and creates conflict in the relationships they have. For example, the cold nature of these people pushes others away. Their interactions stay shallow and lack any real emotional connection. The creation of the Short Dark Triad (SD3) test helps experts study these patterns. This tool shows how these traits predict bad results, like more aggression and less teamwork. These dark traits affect more than just the actions of one person. They change how people interact with each other in their social lives.(Furnham A et al., 2013). Additionally, the development of instruments such as the Short Dark Triad (SD3) has facilitated the exploration of these dynamics, revealing how these traits can predict adverse relational outcomes, including increased aggression and decreased cooperation (Daniel N Jones et al., 2013). Ultimately, the repercussions of the Dark Triad extend beyond individual actions, deeply influencing the fabric of social interactions.
Machiavellianism
Using a person for one’s own gain
Machiavellianism is a main part of the Dark Triad. This personality type uses manipulation and deceit. These people use a harsh way of dealing with others. This trait has a similar base to psychopathy and narcissism. It stays different. It focuses on planning how to use people. It involves being cold and detached. New studies show that Machiavellianism often overlaps with narcissism and psychopathy. This highlights the shared trait of cruel manipulation. This trait defines the whole Dark Triad group. Experts sometimes ignore that these ideas have many layers. This makes it hard for researchers who want to study their links. Scientists can look at Machiavellianism as its own trait and as part of a bigger group. This helps them judge its impact on how people act and mental tests. This detailed view adds to the discussion. It helps people create better ways to help those with these traits.(Furnham A et al., 2013). However, the treatment of these constructs sometimes overlooks their multidimensional nature, presenting a significant challenge to researchers aiming to dissect their intricate relationships (Joshua D Miller et al., 2019). By understanding Machiavellianism as both a standalone personality trait and a part of a broader construct, researchers can better assess its implications for social behavior and psychological assessment. This nuanced perspective not only enriches the conversation but also aids in developing more effective intervention strategies for individuals exhibiting such traits.Manipulative Strategies and Traits
Manipulative tactics are part of Dark Triad behaviors. These behaviors include narcissism, Machiavellianism, and psychopathy. These traits share a core of callousness and a drive to control other people. This focus often leads to poor social and mental results. Studies find that people with these traits often use lies. They manipulate others to help themselves and do not care about the well-being of others. These traits overlap in complex ways, and that makes it hard to judge a person. For example, narcissists use others to protect their own self-esteem. Machiavellians use these tactics for their own benefit (). Other research links these traits to low levels of agreeableness. This shows a clear lack of care for getting along with others (). Learning about these tactics helps us understand the broad effects of the Dark Triad on social groups.(Bundy T et al., 2017)). Furthermore, research highlights that these traits are significantly correlated with lower levels of agreeableness, indicating a pronounced disregard for interpersonal harmony ((Furnham A et al., 2013)). Understanding these manipulative strategies enhances our comprehension of the broader implications of the Dark Triad on social dynamics.
Role in Social and Occupational Contexts
The Dark Triad of Psychopathology includes Machiavellianism, narcissism, and psychopathy, and these traits affect how people act in social and work settings. People with these traits often manipulate social situations to benefit themselves. They find short-term success but often damage long-term bonds and workplace peace. Research shows high levels of Machiavellianism and psychopathy cause job performance to drop. These traits break down team unity and lower output. The ways these people interact involve cold manipulation. This behavior ruins relationships and changes the office culture. Understanding these traits helps reduce their impact on the workplace and build better social habits.(Ernest H O’Boyle et al., 2011). Furthermore, the interpersonal strategies employed by those with Dark Triad characteristics reveal a common thread of callous manipulation that not only affects interpersonal relationships but also shapes workplace cultures (Furnham A et al., 2013). Consequently, understanding these traits is essential for mitigating their impact on organizational environments and fostering healthier social interactions.
Conclusion
The Dark Triad represents a very dangerous person at varying levels. Please also review AIHCP’s Healthcare Certifications
The Dark Triad of Psychopathology includes Machiavellianism, narcissism, and psychopathy. Studying these traits shows us people’s actions. We see how they treat each other. These three bad traits are different, but they all involve mean ways of using people. Psychologists must use precise tests to study them. Research, like the work by Paulhus and Williams, shows these traits. They share some features and link to their own mental results. Experts made fast tools like the Short Dark Triad (SD3) for researchers and doctors. These tools are precise. They help us see these traits in local groups and clinics. We can learn about bad behaviors and their effect on society by looking at the Dark Triad’s meaning.(Furnham A et al., 2013). Moreover, the development of efficient measures like the Short Dark Triad (SD3) underscores the importance of reliable assessment tools for researchers and practitioners alike, allowing for a comprehensive understanding of these traits in both community and clinical settings (Daniel N Jones et al., 2013). Ultimately, addressing the implications of the Dark Triad can enhance our grasp of maladaptive behaviors and their impact on society.
It is also crucial for individuals to understand the dangers and signs of meeting these types of individuals. They can be quite charming at first but overtime, the fake mask is removed.
Summary of the Dark Triad’s Influence in Psychopathology
The Dark Triad includes narcissism, Machiavellianism, and psychopathy. These three traits help us understand the field of psychopathology. They relate to antisocial behaviors and problems with social connections. Research shows these traits link together and are common in men. They show a concerning link to negative social results like conflict and aggression. The shared core of callous manipulation among these traits reflects a pattern of bad behaviors. These behaviors challenge old ideas about personality. The findings show we need better ways to measure these traits. We must look past simple tests to see the full picture. We need a broad look at how they affect mental health. The effects of the Dark Triad appear in clinics and other psychology fields. These complex patterns require more study in future research projects.(Muris P et al., 2017). Moreover, the shared core of callous manipulation among these traits reflects a broader pattern of maladaptive behaviors that challenge traditional personality paradigms (Furnham A et al., 2013). These findings underscore the necessity for nuanced measurement approaches that capture the complexity of these traits, moving beyond simplistic assessments to embrace a more comprehensive analysis of their influence on psychological health. Ultimately, the implications of the Dark Triad’s dynamics extend into both clinical and applied psychological realms, warranting further scrutiny in future research.
Implications for Research and Mental Health Interventions
Researchers study the Dark Triad, and this group includes psychopathy, narcissism, and Machiavellianism. This work helps science and mental health care. The field of study has changed over the years. Treating these traits as one simple thing is a mistake that makes therapy less effective. Experts use proven psychological models to study these traits. This work helps us see them clearly. It leads to treatments for their cruel and tricky core parts. Researchers are now building better ways to measure these traits. These tools help them separate overlapping parts of each trait. This data helps doctors choose the right therapy for their patients. It makes treatments work better for people with Dark Triad traits, and this care leads to better results in mental health care.(Joshua D Miller et al., 2019). Moreover, examining these traits within the framework of established psychological models promises to refine our understanding, potentially leading to targeted interventions that address their callous-manipulative core (Furnham A et al., 2013). As researchers develop more comprehensive measurement tools and methodologies, the capacity to disentangle these overlapping variables will improve. This clarity can help clinicians tailor therapeutic approaches, thereby enhancing the efficacy of interventions aimed at individuals exhibiting traits associated with the Dark Triad, ultimately fostering more constructive outcomes in mental health care.
The secular world voices concerns over many types of planning. Financial planning dominates most venues as critical to one’s security and future retirement. Commercials flood the television with various firms that can assure oneself and one’s family’s future through the guidance of financial advisors. One also sees the shift of importance to health and dieting, as well as intense workout plans. Life coaches, personal trainers all help create unique physical and dietary plans to the needs of one’s personal goals and health number parameters. Such concern over health and financial security is important and should be on the top of everyone’s list but in the secular world, seldom does one hear of spiritual planning. If one’s bodily health, or financial security or stability of one’s retirement in the temporal realm is important, where is the more pressing concern of one’s spiritual health, spiritual security or heavenly retirement? In the secular world, as St Teresa of Avila points out, so many exist outside the interior castle of the soul and its inner monologue and relationship with God. The soul is so blinded by the needs of the body that it forgets itself. Instead it ONLY sees the needs of the body, its health, its security and its future at the expense of the soul’s eternal salvation. When imbalance of such exists, then these physical goals and planning become illusions and false idols that detract from one’s final end. This is a very perilous life style.
Spiritual planning based upon God’s will is key. Spiritual planning should be as primary a concern as any financial planning. Please also review AIHCP’s Christian Counseling Program
In this blog, we will look at Spiritual Planning and how to implement some the most basic elements of it to provide spiritual growth and stability and a closer relationship with God. In this blog, our financial planning is interest in grace not money, growth in virtue not assets, security in God not bonds, and retirement in heaven not Florida. This blog in itself could be a long manuscript on such a broad subject, but will attempt to keep the subject as compact as possible with also consideration to other blogs and concepts, as well as texts, within AIHCP Christian Counseling as well as Spiritual Direction resources that have already touched on similar concepts found in this blog.
It is imperative for Christians to remember that salvation is not an accounting book of one’s own good deeds versus bad deeds. One cannot live a sinless life. The fall of Adam has prevented such endeavors and as broken human beings, we need the grace of God, earned through His Son on Calvary for salvation. One’s faith in Christ is essential for salvation, for one cannot find salvation in one’s own works. Pelagius, an early Church heretic, attempted to heretically teach that one’s human nature was not completely corrupted and that one, albeit rare, could imitate Christ and possibly live a sinless life. Pelagius believed works could save oneself. This was condemned by the Church at the Council of Carthage, and equally rebuked by the great saint, St. Augustine. St Paul indeed teaches that it is through Christ and His death and one’s faith in Christ that souls are saved, but it is important to understand that faith is more than a formal assent, but is a cooperation with the graces earned by Christ at Calvary. Christians are not saved by faith “alone” which was never included in the original translation but through faith which encompasses a working nature. Scripture emphasizes a working faith in Christ that balances the assent of faith with its fruits and works, for St James emphasizes the balance of spiritual works in faith. Christ, Himself, commands His followers to keep His commandments.
Hence as Christians believe that one cannot earn heaven by oneself, as if balancing a ledger, but one must completely rely on the grace earned by Christ, at such a high cost for each of us, for one’s salvation. The fruits of the working faith, the cooperation with the grace earned by Christ for one’s salvation, does not belong to oneself but a when connected to Christ, and under the grace of the Holy Spirit, become salvific. Spiritual Directors, as well as Christians who attempt to better themselves in spiritual life, must first come to this ultimate surrender that their salvation is not their own but a gift from Christ and applied through the Holy Spirit. The Blood of Christ cleanses one of sin and pays the price for that Original Sin of Adam as well as the actual sins committed by oneself. Alone, no matter what one does, like the past sacrifices of patriarchs, are insufficient, but when aligned with Christ and His death, where one’s cross becomes tied to Christ’s cross, then they become pleasing to God. Christians are not activators of their salvation, nor are they passive recipients of it, but are cooperators with what was earned at the cross, motivated by grace to the gift of salvation.
The Spiritual Planning strategies in this blog do not replace Christ’s gift of salvation, but are grace motivated gifts of the Holy Spirit to participate in that redemption at a more efficient way. While the soul participates, it is the grace of the Holy Spirit that encourages it, strengthens it and molds it. Unlike physical fitness and planning, where one plays a key role in physical transformation-albeit guided and trained by another, the spiritual transformation of a soul is the work and grace of the Holy Spirit.
It is important then to find humility upon any spiritual transformation-for all virtue and grace come from the Holy Spirit that was earned by Christ at the cross. One must come and apply the Blood of Christ and Grace of the Holy Spirit, but it is not one’s own deeds and actions but the work of God existing within one’s faith that permits such a cooperation. So, like all endeavors, one must be mindful of pride. Like financial planning, or physical training, pride can easily corrupt a healthy self image with vanity. Likewise, in spiritual transformation, pride can create the illusion that one has made oneself holy and that one is more holy than other people. Like the Pharisees, one can have one’s own spirituality become a weapon and tool for one’s own damnation. It is so important as one enters into a deeper relationship with God to be mindful of spiritual pride and to pray daily for continued spiritual humility and complete reliance on the grace of God. Salvation and faith is a gift from God and something earned by Christ. We are merely partakers of this gift and must always give honor and glory to God for any spiritual gifts or insights. With this understanding, the remainder of this blog will look at some helpful techniques in spiritual planning and growth.
Spiritual Planning
Supplied with the grace of the Holy Spirit to transform purely human thoughts and deeds into something more, one can work with those graces to better obey the commandments, submit to God’s will, grow in virtue, and enter into a deeper and more healthy relationship with God. This direction and progression towards God is a life long process with pitfalls, crosses, joys, successes, failures and losses. However, what it needs to be is a progression and a perfecting of oneself in virtue to have a deeper relationship that translates into the next life with God. Padre Pio points out that progression is key. A soul, even one that has sustained growth, that fails to continue in growth or progression becomes stagnant. The soul, like a plant seeking light, must continue to grow in the direction of that light, guided by the light and nurtured through it. The moment the soul stops seeking that light, it ceases to grow in communion with God. One can consider the temporal analogy of financial growth. If one has grown in wealth and has seen continual growth in the one’s accounts with a health market, then suddenly notices a stagnant level of return, there would be great concern. Why not for the soul? If growth has suddenly stopped or become stagnant with relationship with God, this should be a serious concern. For instance, a soul that regularly attends service in Protestant churches or Mass in Catholic churches, but has no spiritual connection despite obligatory attendance has entered into a state of concern. This is why Padre Pio reflected the vital importance of continual growth, despite setbacks, but continued renewal. If a soul falls, does it immediately seek God’s forgiveness? If one fails, does one immediately identify the issue and rectify it? As sinners, we all fail, but what is critical in spiritual planning, is not only the “attempt” to limit failure, but one’s quickness to rectify it. This again stems to one’s insight on humility and pride. If one understands one’s nature as broken, then one who falls, falls in humility but also seeks forgiveness in humility. One in pride who falls, has a far harder time seeking forgiveness.
All spiritual planning requires grace for we cannot earn our salvation. Spiritual planning is participating in that grace
Spiritual planning must acknowledge the reality of failure, but it almost acknowledge the life long nature of the journey. In life, some look for quick investments without securing a solid foundation. Others in physical training, desire a physique but lack the discipline to attain it. Some who diet, see a diet as a temporary status to attain a particular weight to fit in that dress, instead of a life long purpose of dietary health. Spiritual growth is not fast, it is not temporary, but it is a life style. It not likened to a New Years resolution, or a Lenten journey. Lent, for many Christians, is a spiritual diet. It lasts 40 days and then is suspended after Easter. The spiritual disciplines of Lent should be intensified in unison with the Church and in memory of Christ’s passion, but it should not be a spiritual diet for 40 days. The experience of more prayer, Scripture, introspection, fasting, denial, sacramental experience and spiritual growth in virtue should not be a 40 day experience but should represent the base line of all Christian life. This is not to demean the naive view of Lent by some Christians, for it is far better to sense some need than none at all, but, as Avila points out, these souls represent the utmost basic relationship with God and His grace. They, like a first level mansion, walk in, walk out, may peek inside its windows, but fail to grasp the greater beauty further inside the interior mansions of relationship with God. They become distracted by the lures of the world and progression spirituality ends abruptly until a later existential emergency or spiritual feast day.
Spiritual Planning is a life long journey that is about constant growth, humility in that growth, acknowledgement of failures, and complete trust in the grace of God to allow one’s working faith to manifest fruits and a closer relationship with God; A relationship that manifests in its finality in Heaven with God.
Spiritual Planning Ideas
Counseling strategies, life coaching, and physical training plans are quite similar to spiritual training. As Mark Walberg commonly states, “Are you prayed up”. Spiritual Directors are Spiritual Trainers in this sense. They are not just spiritual but also should have a core understanding of counseling techniques based in goal setting and facilitating change. In previous blogs, we discuss the psychology of change and habit. We discuss neuro-pathways and how habit takes time to form. One does not suddenly become a a horrible sinner by one trip nor a great saint by one wonderful moment, but it is a character and progress of that character that defines both virtue and vice. As the ancient philosophers noted, character is a continual presence of a particular excellence in action that is unhindered but natural to the nature. This is natural habit is not something easily gained, or lost. One merely can look at the horrible nature of sin and its addiction itself. One who works to rid oneself of vice must work with the grace of the Holy Spirit to heal, change and transform. God can miraculously change and convert a person, but in most cases, the journey is one of a cross, one where one’s nature learns of the love of God and His continual mercy as change is undertaken and achieved. So, suffice to say, the process of change involves counseling. It involves goal setting. Just like certain financial goals are discussed, set and hoped for, so certain goals spiritually must be discussed and planned. Like exercise, the goals of a certain weight, or certain amount of reps in a particular weight training, concur with a particular habit or virtue that one aspires for. As meticulous journals keep weight training numbers, so one may need to keep track of one’s modified behavior in recollection and examination of conscience. How many times, did I sin today? How many times, did I accept the grace of God and overcome temptation? St Ignatius Loyola in his spiritual exercises in week one, challenges the person to almost scrupulously monitor and track one’s failings. As if tracking calories, St Ignatius asks us to track sin and vice! A working faith demands such accountability to a God who has paid such a high price for us and has made such graces available to the soul for its salvation.
Goal Planning
Goal planning is part of the counseling paradigm. This is especially seen in behavioral therapies where behavioral change is based on how one thinks. Behavior is greatly modified and altered by how one thinks. Cognitive Behavioral Therapy helps individuals think differently so as to feel differently and finally behave differently. Within the behavioral model, desired changes take time but they are planned changes in behavior starting in how we think about things. Spiritual Directors can help individuals think differently about life through the prism of grace, God, and virtue. In doing so, desired behavioral modifications as well as targeted virtual habit can be set in goals.
Like all behavioral modification, spiritual change shares common counseling goal setting strategies
Again, though, before any planning can be undertaken, unlike temporal planning which relies on the strengths and powers of oneself, spiritual planning must be placed entirely into the grace of God. Goals and noble desires are attained through grace and normal actions are spiritualized and made perfect when united with Christ. Hence no spiritual plan can have any value if placed in pride and self or the belief that one’s own works and deeds have value without the guidance and grace of God. Without God, these works, dreams and aspirations are utterly worthless. This is why any plan, before undertaken, must be placed within the guidance and protection of God. Daily prayer, devotion, and commitment to God’s will is essential. When one rises, all plans, all duties, all vocational assignments, all crosses, and all joys must be given to God. The morning offering gives to God everything one does in a day before the day starts and unites everything to Christ to be offered to the Father as a perfect sacrifice to be guided by the grace of the Holy Spirit. One must then relinquish control and unite one’s will with God. One must acknowledge one’s utter dependence on God and again unite one’s will to Him for transformation. Placing one’s plan under the guidance of God and allowing it to fall under His will is a big differing point between temporal planning and spiritual planning, but for the Christian, why not submit all plans-even temporal- to God’s will!
In counseling, especially behavioral therapies, plans need to be discussed and identified. The goal need identified but also how to attain the particular goal, the challenges to that goal, possible setbacks and time frames. Because of the human nature, the counselor needs to curb enthusiasm so as to prevent burnout when goals become difficult. Great zeal can quickly turn to great despair. The counselor is trained to set intermediate goals for a person. Little goals that track progress can help build confidence and lessen despair upon failure. This can be seen in financial expectations, as well as weight loss expectations, or even behavioral modifications to stop smoking or drinking. An individual with a spiritual plan to evict a vice from one’s habitual orbit, may find despair if one fails on a particular day. Like a person who succumbs to a cigarette or donut late at night, one can succumb to a vice. A good spiritual director can calm the person and identify why and how it occurred but also to remind one that habits take time and goals take time to achieve. One needs to find mercy in God when one fails and not find complete pride or joy in one’s own accomplishments but to reflect all in God.
Pitfalls are part of all plans. Individuals attempted to escape habits, fall, but what God cherishes is the choice to change and the direction. This is why spiritual directors should encourage the soul and point out the importance of gradual change in severity and frequency and the mercy and grace of God. Intermediate goals do not demand perfection but gradual growth. Once intermediate goals are met, one can move forward to the next step. Like weight training, once a certain number of reps are met, or a certain weight is attained, one is able to advance. Like so in spiritual life.
Like all planning, it is crucial to keep the person focused but also humble and also remind one of one’s nature. Many times during change, individuals become obsessed more so with the numbers than the journey and end goal. One can become scrupulous and focus more on avoiding or worry or fretting over the smallest of actions to the point it causes extreme distress, despair and guilt. The devil can be very subtle in derailing a soul working towards God. So it is important that whichever habit, or spiritual goal one has, to not mistaken the goal or new habit as the ultimate end. Unlike the view of the ancient philosophers, virtue itself is not the end goal of our worship. Virtue is a vehicle and intermediate step to the ultimate goal which should be relationship with God. So when one focusses more on numbers, one begins to focus more on self than God. God is the ultimate goal in the entire endeavor of spiritual planning. Unlike physical training, when one only looks at the body and its change, but not the overall health, then derailment can occur to various maladies. Likewise, when virtue is sought for the sake of virtue, instead of its purpose as a vehicle to God, then it can be turned against oneself. In this, one needs to see things that are means as means, and clearly in planning contrast it with one’s end. Counselors help individuals navigate this, as well as spiritual directors.
Spiritual Strategies
With a stronger understanding of the nature of planning, as well as setting goals, and understanding the difference between means and ends, we will quickly review some types of spiritual plans. In my daily life, I believe in planning. Calendars are essential but also journals as well as notes to self, as well as self talk to keep one on track. Life is comprised of professional, academic, family, self, physical and spiritual aspects and we need to balance these in accordance. We need to structure these vocational duties that we owe to God, self and neighbor. First and foremost, they must be prioritized. Certain things on lists are non-negotiable. They are priorities that must be met before others. Obviously physically, diet, grooming, and sleep are among those. Spiritually, prayer, worship and communion with God should top that list. However, in any planning, there are events, assignments, or obligations that are secondary to primary ones. Some may be flexible and able to be moved, while others may be optional. It is important to define these when planning.
Spiritual strength involves not only God’s grace but also an active participation of developing spiritual habits. Please also review AIHCP’s Christian Counseling Program
Planning wise, like financial plans, I like to plan by the quarterly year. While I have daily duties, weekly duties, bi-weekly duties, and monthly duties, that lead to fulfillment of the quarter, I like to see set goals for that period. Some goals are primary, others may be flexible, but they are listed. The 3 month period serves as a reminder of what needs done in some cases, but also where I would like to be as a measuring stick. Obviously one can see where this can be applied financially, physically but also spiritually.
From a spiritual context, how has one’s daily, weekly and monthly habits gradually changed over the 3 month period? Daily journaling, weekly remarks and monthly checks can keep one on pace with possible goals. If one is stricken with the vice of drunkenness, one can review the number of drinks a week and its gradual reduction from week to month to quarterly period. If the goal is to reduce this habit, then one may discover a new trend that one can find solace in as recorded numbers show reduced intoxication as well drinks per week or month. One can then ascertain if one has met the quarterly goal or not and how to access the next quarter. Remember, this is a life style, it is a marathon, not a race, so gradual is better than nothing. This again takes one to the importance of daily and weekly monitoring, so that data and change of habit can be documented. During this examination of conscience, at the end of each day, or week, or month, or every one quarters, one can see the weaknesses, what one can do better, and most importantly remember on one’s complete reliance in God for any change. The spiritual director can encourage the soul in this progress and also help set new intermediate goals, or re-ascertain certain strategies or time tables to help maintain the confidence of the person in this change and ultimate better relationship with God.
The spiritual director also becomes a spiritual coach in this endeavor. Upon reflection of plans, one’s attainment, progress, or failures, a coach helps develop a person’s skills. This may consist in different prayers or penances, or fasting that help foster a particular virtue or habit. Particular spiritual readings of the saints and their writings, as well as Biblical books or chapters that correspond with one’s troubles can be utilized. Goals within a particular time table may include within a 3 month span to work in charity, or read a certain amount of books, or become more acquainted with a particular book of the Bible that will help one move forward. In may also include if Catholic, more frequent reception of the Eucharist, as well as confession. These things not able help the soul in despair, but also give the soul sources of grace to help transform over the spiritual planning time. Spiritual directors or confessors can become original in their ideas to share with individuals various particular deeds, or readings that meet a person’s needs and direction.
With all planning, one seeks change, and good change agents produce change. This involves within the spiritual planning, promoting healthier communications and removal of vice associated materials. These things that promote sin are referred to as occasions of sin. It can be a person, place or thing. Spiritual directors need to encourage souls to avoid places associated with particular sins. If bars are associated with drinking or lewd conduct, then these places should be removed from a person’s habitual visit. The same holds true for any addict of any vice. In regards to lust, avoiding imagery or situations that promote lust should be removed from one’s life. If a cell phone in close proximity calls one to pornographic imagery, turn off the phone or remove it from one’s reach. Many of the saints practiced far greater mortifications, beyond what I would recommend, but one must, if seeking change, remove the occasions of sin. Like a person a diet who removes donuts and cakes from the cabinet, one must remove occasions associated with the detrimental behavior.
Like wise positive change agents must be introduced into any spiritual plan promoting change. Like in a diet, one supplies their refrigerator with wholesome foods, so the soul must supply the daily routine with wholesome content. Good spiritual reading, better company, prayer, as well as support from other religious persons who share the same ends is crucial. A clean home promotes change, so does a clean spiritual environment. One needs to remove the spiritual filth for the soul to change. Like a dirty body that needs cleaned to become healthy, so does a dirty soul need cleaned to move forward. Christ’s blood and the grace of the Holy Spirit provides the solution. One must wash oneself in these things and provide oneself with healthy reminders of those things that promote new spiritual change within oneself. Healthy and positive change agents replace negative occasions of sin and replace maladaptive coping with healthy spiritual coping founded in prayer and faith in God.
Conclusion
Spiritual planning is a life style change that takes time and is a life change of progress towards God. One cannot earn this change but it is gift from God that we partake in. While the grace of God is a gift, one still must work with that grace. Spiritual change, like any change, or plan in life, is something that one must dedicate oneself to and purposely plan to achieve with commitment and guidance of the Holy Spirit. There are many ways to promote a better relationship with God and when we find time to plan prayer, worship and submission to Him, He will guide us in all our plans to find better communion with Him.
We should plan ahead spiritually and work on our relationship with God as much as we do with other types of financial planning or health training. Please also review AIHCP’s Spiritual Direction Program
Spiritual planning in itself should be a big part of one’s life. It should take priority over everything else we do because our ultimate end is God. Spiritual planning acknowledges the necessity of Christ’s death and the grace for salvation and how to apply it to our lives so when we stand before God, we will know Him well, as we enter into paradise.
Routine assessment of vital signs and visible symptoms. These two are by far considered to be the most common indicators of a patient’s improving or worsening state. However, healthcare professionals are blessed with something commonly known as ‘intuition.’
In many cases, it is this abstract and powerful force that helps recognize signs of deterioration. Exercising intuition and discretion is crucial, as they often decide a patient’s fate. This is especially true of those who do not fit into the regular criteria for high-risk patients.
Do not fret if you also struggle in this area. This article will help you by sharing three signs of a patient requiring extra vigilance. They will help you prevent complications and ensure patient safety.
Changes in Patient Narrative Over Time
Charts and lab reports may fail to provide the answer that patient stories can. Alexandra Dubois, Senior Vice President of Patient Engagement for OPEN Health, says, “You have to honor the lived experience as a form of expertise.”
It is indeed true that key opinion leaders and healthcare providers are often viewed as the best source of information. What needs equal, if not more, importance is to overlay the patient perspective.
Storytelling is a powerful tool for patient communication. Since the narrative is usually emotional, it has the power to make a difference. Therefore, it’s a major sign that a case may need extra vigilance when a patient’s symptoms or cause of injury change over time.
Now, changes do not automatically mean something is wrong. They may even affect the way a patient talks about their experience. A national analysis of over 65,000 medical malpractice cases found that 20% of them involved at least one documentation failure.
Precise records are important, especially amid changing patient stories. So, what would good practices include? Look at the following:
Write down patient statements clearly, even word-for-word.
Note the time each new detail or symptom was reported.
Avoid falling into assumptions about cause or intent.
Let the care team know about any changes.
Finally, even seemingly trivial changes in a patient’s symptoms often become useful clues to complications that may not have surfaced yet. A patient with mild pain in their abdomen may complain of similar discomfort in other areas.
Simple as it may seem, such changes point towards underlying physiological issues or delayed side effects. Healthcare will only have the upper hand when changes in the narrative are tracked over multiple visits.
Increased Requests for Detailed Records
Every patient and their caregivers have the right to access health records. However, ongoing scrutiny may mean that the case requires extra vigilance from healthcare professionals.
This doesn’t always translate into formal submission of records. Some patients may be highly critical, and their family could make repeated requests for clarification and details. For instance, in Colorado Springs, a city with a growing population of military families and outdoor enthusiasts, healthcare providers frequently care for patients recovering from accidents or injuries.
Many of these patients are involved with critical documentation procedures, particularly when they sustain injuries due to someone’s negligence. In such cases, they often rely on a Colorado Springs personal injury lawyer for guidance after the incident.
As the Springs Law Group notes, Colorado has specific laws related to auto insurance requirements and negligence that a local attorney understands. Even in such cases, the healthcare provider’s role remains clinical, but precise documentation is a must.
As per 2024 national data, nearly two-thirds of patients in the US accessed their medical records online at least once. Many were repeatedly viewing their portals or verifying details. Patients who are critical or detail-focused often behave this way.
Patient vigilance is one side of the story, but these situations demand no less from licensed healthcare professionals. For the latter, extra caution would imply the following:
Maintaining clear chronological documents
Recording patient statements without interpretation
Clarifying instructions in a professional and neutral tone
Sharing updates with the care team
Growing Emotional Distress in Clinical Settings
Healthcare professionals often come across patients whose emotions tend to become very volatile after a serious illness or injury. Traumatic Brain Injury (TBI) is one relevant example. It can affect emotions, especially when areas of the brain controlling emotions are impacted.
In most cases, anxiety is among the first noticeable effects. Now, that’s not merely an emotional response. As per a 2025 survey, 40% of the participants experienced moderate to severe anxiety levels. Some of the contributing factors were health uncertainty, misinformation, and a perceived lack of control.
Why would any changes in emotional or behavioral intensity call for extra vigilance? For starters, there are risks like medication errors or missed follow-ups lurking on the horizon.
Anxiety also has its way of altering communication. On the surface, the patient may be acting “difficult,” but it could simply be the only way they know how to cope. Most importantly, what if anxiety impacts physiological recovery? In most cases, the mind and the body are interlinked, so you cannot neglect one without risking the other.
Now, it’s vital to know which signs may be ignored and which require immediate assistance. Listed below are the signs that demand extra vigilance:
Repeated requests to restate or reword previously communicated information
Rising frustrations regarding symptoms or treatment plans
Regular demands for written confirmation of findings
The minute emotional responses intensify, healthcare practitioners must communicate in a calm and neutral way. If anything, avoid absolute statements and speculative comments about prognosis like the plague. Simply segregate what’s been clinically confirmed and what awaits further evaluation.
Healthcare providers must remember that even the smallest details can reveal important aspects of a patient’s care needs. In England, more than 800,000 patient safety events were recorded between July and September 2025. Many of these cases involved near-misses and preventable issues.
Since subtle signs can have drastic implications, healthcare teams must always be on the lookout. Being paranoid is unwise, but turning signs into means for safer care? That is exactly what keeps patients safe and care practitioners a step ahead in the industry.
Author Bio
Deepika is a budding content creator who enjoys exploring various niches, be it lifestyle or healthcare. With a knack for breaking down complex topics, she strives to make information relatable and accessible to everyone. During her leisure, Deepika enjoys reading novels and practicing fine arts to keep her creativity alive.
Please also review AIHCP’s Health Care Manager Certification program and see if it meets your academic and professional goals. These programs are online and independent study and open to qualified professionals seeking a four year certification
There are many different interpretations of verses in Scripture about God and His justice and mercy. Pending on the era of time, you also have different theologians, saints and mystics expressing within God His justice or His mercy. Sometimes, one can review readings from a particular saint that produces a harsh and fearful tribunal seat of God, while others will show a loving and caring father. Even in modern times, Christianity seems to present a dual image of God. Progressives shower one with the idea of God’s infinite love, while more conservatives display a law bound God who judges and condemns. It is very important not to overweigh one attribute over the other. If one only focuses on justice, then only a half truth emerges, which only a refocus on God’s mercy can balance into the fullness of the truth. The reality is God is both just and merciful but various interpretations from Scripture or beliefs of saints and their writings can lead one to have an imbalanced spiritual view of this. Either one that is constantly fearful, or one who is too careless with the joys of the world. In addition, how God is viewed through human lens plays a big role. Scripture presents many images of God and some can be distorted when taken too literal or for that matter entirely dismissed. Anthropomorphism is common literal device used in Scripture. In these cases God can be given many human like attributes in regards to His emotional reactions to human activity as well as images as a judge in the strictly human sense. These images need to also be properly understood in context as well as symbolism to have a greater understanding of God. This blog will look at some of these realities and attempt to balance them in proper measurement in correlation with Partial Judgement of a soul who goes to Heaven or goes to Hell.
There is a balance between God’s mercy and justice. Please also review AIHCP’s Christian Counseling Certification
God: The Loving Father of the Prodigal Son or The Fierce and Avenging Judge?
The two images above create quite a contradicting imagery but both do point to truths but when not balanced become partial truths. So many times, preachers, priests, or pastoral leaders, and even oneself finds one particular imagery of God that is superseding over all others. One’s own experience can play a large role. Spiritual individuals are attracted to certain images of God in Scriptures because it meets a need or answers an existential question that is pertinent to oneself. One’s own mental and emotional state also plays key roles in which imagery of God best fits our current need. Those who suffer from low self-esteem, or have attachment issues due to past trauma live in a state of anxiety and that state of anxiety can play a role with their relationship with God. Person’s in such mental states may have a greater fear of God, or complete imbalanced feeling of unworthiness. They may also see God as a more fierce and avenging judge. Others with a more delicate conscience or scrupulous conscience may be tormented with obsessive compulsive disorder and see God more as a judge who keeps score on the day of judgement. On the other spectrum, those who live life carelessly may need to see a parental God that dismisses foolishness and error as if it does matter what one does in life. They need a God who does not reprimand sin, but a God who only sees love. In their mind, their love of others and overall good human nature is enough-“God will not judge me but only loves me for who I am!” As one can see, these are two equally dangerous routes. Both capture an element of truth, but without each other complimenting each other, the fullness of the truth is lost.
As seen in Scripture, despite literalism or symbolism, we see a balanced approach that displays both sides of God in different books. In the parable of the Prodigal Son, one can see the untamed and complete compassion the father has for his lost son. The father never gives up loving the son and upon the son’s return, offers complete forgiveness and restoration to the son. In other imageries, one can see God as a terrifying judge who he sends souls to Hell, and casts these souls into the abyss of the wicked. The words are strong and harsh and helps illustrate the extreme disgusting nature and true evil of sin. Christ originally came as a Redeemer, but in Revelation, He is also a judger of humankind, separating the goats from the sheep. Such strong phrases as “depart from me” and “cast into Hell for the fires prepared for the wicked” all show this other side of God and Christ when judgement arrives for a soul.
Ultimately, if one wishes to truly understand God’s justice and mercy, one must understand the expression of Scripture and its aim in its full context and not individual quotes. One must be careful to avoid cherry picking of verses out of context of the chapter or theme. In addition, one must closely interpret symbolism to avoid sometimes literal interpretations that promote an anthropomorphism of God which gives Him human qualities of revenge or rage. Also, one must understand other saints or mystics interpretations of God’s justice and mercy pending on the time period they wrote and the type of language that was used. Many times as well, saints wrote in particular styles to promote one theme of God and these writings can at times seem imbalanced, especially for individuals not trained in pastoral ministry and theology. A particular saint may be illustrating God as judge and the disgusting nature of sin which can terrify a delicate soul but also at the same time promote enough self inspection and fear for a soul to change. As well, a particular saint may present writings or mystical visions that portray the totality of God’s love and the immensity of it. This may be good for a more spiritual stable soul but a message that would be dangerous for a soul who has no boundaries with sin.
In essence and answer to the leading question, God is both loving Father and fierce Judge but how one understands the true dynamics of it from a theological standpoint is essential to avoid literalistic pitfalls that can lead to scrupulous and constant fearful behavior or lax and boundless carefree behavior.
Moral Theology and Sin
Pending on one’s image of God, incomplete truths can distort one’s views on sin, but it is only when one accepts the full imagery of God, can one see the full picture of sin, self and union with God. First and foremost, Original Sin or the sin imparted on humanity after the fall of Adam, left humanity with a broken nature. The gifts of great knowledge, stronger mind and body connection and control of the passions imbedded within Adam’s character were an abilities his descendants never experienced. Through Christ’s death and application of His graces through Baptism, one again enters into full communion with God and one’s soul becomes alive through Sanctifying Grace. This however did not restore the fullness of human nature. The temporal reality and the consequences of the sin left a scar that was not wiped away after Baptism. Humanity while redeemed still was broken. While Christ reopened grace and a relationship with God through His death, the temporal reality left individuals open to sinning. Personal sin could then undo the bond of Baptism. Certain particular sins could even cut grace off from the soul. In this state without remorse, a soul again became distant from God.
St Ignatius Loyola exercises helps one examine their conscience and reflect on the justice and mercy of God
St Ignatius Loyola in his Spiritual Exercises describes sin as disgusting and deforming. Like a tumor, it tears into the soul, disfiguring it. Any sin rejects truth and the love of God. Sin is choosing self, or others over God and rejecting God’s authority. St Ignatius in his exercises challenges the soul to identify sin, to meditate on its grotesque form, and to imagine the state of a soul in mortal sin that rejects God’s love. He asks one to consider God as judge, but he also reminds us of God as father who loves. However, for whatever particular reason, in many of his meditations within the exercises, one solely focuses on God as a fearsome judge and the total worthlessness of the human person in comparison to the greatness of God. One is asked to meditate as one being a condemned criminal before a judge, as well as meditating the pains of Hell and the danger of one mortal sin. Much of this has to do with shocking the system into understanding the damage of sin and to induce a holy fear of Hell, but also a disgust for sin and a love for virtue. It also focuses to show how utterly dependent one is upon God’s grace to avoid such vile sins.
Sin is hence a great disorder and injustice itself towards God. In this way, all personal sin shares the same substance in that it damages one’s relationship with God. While all sin shares in this horrific substance, not all sins are equal in degree or depth of brokenness. It only took one sin to tear a division between God and man that Christ restored. This alone shows the vile taste of one sin and its shared characteristics but Moral theology helps one to better categorize sin, understand its objective nature, its degree, as well as the subjective interplay a sinful act has with the conscience and circumstances surrounding the agent or person committing the sin.
Personal sin is rightly divided into venial and mortal. Like human laws, degrees of severity of an offense are measured and consequences detailed through different levels of fines. A person who steals out of hunger sins differently than a person who steals from the poor. All is sin, all creates a barrier, but the level and depth of the barrier is measured by the basis of the severity of the offense. A person who commits a traffic violation remains still a good citizen despite his lapse in judgement of speeding, but an individual who murders, pillages and rapes, commits a far more grave offense to society and no longer remains a good citizen. Within the Mystical Body of Christ, offenses hurt, but the degree and multitude of the offense play a key role in whether the soul still loves God, possesses grace and remains attuned to God’s will.
Hence all sin is objectively disordered but the levels of disorder in regards to the relationship between God and the soul differ on severity. Objectively any sin remains a sin within itself. No subjective reasoning or indifference can mitigate the nature of an disordered act. The level of disorder can range objectively but the consequences of the sin can vary greatly beyond its objective label. The human act is more than a black and white event but something with multiple layers of grey. There are numerous subjective elements at play within the act of a sin. First and foremost, what is the intent of the agent committing the sin. Is the person free to act? Does the person fully intend to commit the act? In committing the act, is the person clearly articulating the acceptance of this act and all its consequences? In addition, what biological factors, psychological disorders and uncontrolled passions are at play that weaken the will? Is this act isolated or a continuous habit? Is this act done without remorse or guilt? Does one fully through this act wish to disown God? What other circumstances exist around it? Sometimes actions can become neutral that are otherwise naturally sinful-for example taking a life to defend one’s own life. What other external pressures existed? So in many cases, an objective action that is disordered possess less consequence for an individual based on other criteria.
Padre Pio saw the danger of any sin. Sin weakens union with God. Consistent sin wears one’s soul down and weakens it for greater infection. Padre Pio understood that a soul who goes to Heaven or to Hell does not randomly commit a grave sin and chooses Hell but that a soul gradually chooses Heaven or Hell over a life time. What one is when one stands before God is what one created oneself to be through a life committed and developed through virtue or vice. Habitual sin and lack of remorse leads the soul down the road of rejecting God. This is why it is critical to form a sound conscience that identifies sin as gross and disgusting and a conscience that when one does fall, immediately feels guilt and shame to confess and repent.
God’s Mercy
Sister Faustina reminds us of Christ’s infinite mercy and love
Sister Faustina is most known for her visions of the Sacred Heart of Jesus and His message of mercy. The Chaplet of Mercy as a prayer begs God for pardon and remembers the sacrifice of Christ. It repeats, “for the sake of Your sorrowful passion, have mercy on me and the whole world”. The mercy of Christ and the opportunities given by God through His sacraments seeks for all to be saved. Christ shed His blood for every soul. He shed tears for each soul lost. Many mystics claim this was one of Christ’s greatest agonies–the souls who would reject His passion and grace. Within the Sacred Heart image, Jesus’s Sacred Heart pours out beams of red and white rays from His heart. This displays His infinite mercy to sinners. Like the story of the Prodigal Son, God immediately forgives a soul that seeks forgiveness. This should not be taken for granted though. How many feel they have time to change? Instead of living in the moment, they postpone what matters most.
God’s Justice
God’s justice is referenced throughout Scripture and justice is promised to the faithful. God’s justice while merciful does not permit the wicked to go unpunished. While some may over emphasize this terrifying reality, or over humanize anger and vengeance in the Lord, many need to understand there are consequences of sin. Those who dismiss sin as trivial are led by a lax conscience that does not truly see the disgusting and foul order that sin infects the soul with. God’s standard, His commandments and His laws are not arbitrary but based in the fullness of His own essence. Something is not wrong merely by proclamation for a certain day but intrinsically is wrong for everyone and for everyday. Like evil, sin is a lack of good. It is what God is not. So when one sins, one is committing a grave injustice. Christ’s blood paid the price for sin, but as followers of Christ, we must apply the graces earned through Baptism. As followers one must adhere as best one can to the laws of God. One cannot through one’s own good works earn salvation but it is through faith in Christ and grace of the Holy Spirit that one can follow the laws of God and partake in salvation.
The Divine Judgement
In Christianity, there are two judgements. The Particular Judgement occurs at one’s death bed. The General Judgement is the proclamation and judgement upon all souls. In one’s Particular Judgement, one’s eternal fate is determined. There one sees the balance of God’s justice and God’s mercy. However as discussed early, there are many visual images in Scripture, as well as mystical writings that take these things into account.
One image, as illustrated in Scripture, displays God as judge but in a more human sense. In fact, even St Ignatius in his exercises, portrays an image of God that casts souls to Hell for their wicked deeds. This image emphasizes a strong justice display, with less mercy, but this literal image is an interpretation of that judgement. One can also from a different perspective and interpretation views God as judge from a more theological standpoint immersed in moral theology that balances God’s mercy and justice with the soul.
There are two judgements. Our immediate or particular judgement and the final and general judgement described in the Book of Revelation
One may be amazed, according to Padre Pio, how many souls who seemed evil are not in Hell, and how many souls who seemed so pious are not in Heaven. Only God knows the innermost workings of the soul. As Padre Pio also pointed out, one’s judgement before God is usually not based on one event but a life time of choices that led one to become good or evil or lovers of God, or lovers of self.
Ultimately, God as our moral standard serves as the soul’s mirror at judgement. God does not cast a soul He loves into Hell. The judgement speaks for itself. The soul as if looking into a mirror recognizes what it is in all its good and evil. It is left without distraction or excuses. It is stripped of all the noise of the world and only faced with its true reflection. Did it love God in this world or did it love self? According to Padre Pio, the soul who has rejected God is a soul who will reject God at judgement. It will acknowledge His truth finally but it will reject the truth and its implementation upon itself. The imagery of God casting a soul into Hell in some ways is hence misleading. God finds no joy in this. He loves the soul despite its total corruption but due to His standard, the soul cannot accept. Like the demons and corrupt souls before, the soul in mortal sin rejects God’s friendship, His love and companionship.
Many believe that one is saved by faith alone, but believing in God does not give one salvation. Satan and his demons believe in the reality of God but they are not with Him. The simple act of faith must be energized through the grace of the Holy Spirit to produce charity. This charity varies among individuals. Scripture attests that love can cover many sins. Ultimately, everyone is unworthy of God through one single act of sin, but it is through God’s mercy that saints and sinners alike are made worthy. So, while one’s good deeds are important choices to salvation, one must attest they are never enough. It is ultimately God’s mercy and reciprocal love that is fed through faith and grace that saves the soul before the Partial Judgement. A soul that still loves God, even imperfectly, can not cease loving God. If one loved God on earth till the end, one will love God at judgement. Hell’s greatest reality is the absence of any love. A soul at judgement who goes to Hell is a soul that refused on earth to love God and continues to refuse to love God at judgement. The soul may be well aware of what he is losing but this does not lead to contrition but only further anger , blaming and blasphemy.
Ignatius sometimes appears in his exercises to sow fear of how a soul can so easily lose God and at judgement be cast away by an angry God. There is good reason to mediate upon this, but a soul that loves God, even despite mistakes, even when some sins were in the past mortal, cannot lose God if the pattern of love remains. This entails remorse for serious sin, but God does not send a soul to Hell over a trip or fall, the soul sends itself to Hell for remaining on the ground and never acknowledging the sin or seeking forgiveness. A soul that maintains love of God, may trip and fall in life, but it always bounces back up. That same soul, no more or less than a far more virtuous soul, nevertheless shares one same common theme. No-one meets the standard of God, no mirror can display a an image that makes one worthy, whether mortal or venial, but it is the grace of God that reaches out and if love is returned, then salvation is procured. Learning to love more deeply may be required before standing fully before God, but Christ and His infinite mercy supplies the necessary gap through His blood that ultimately saves the soul.
What makes a soul choose Hell? Please also review AIHCP’s Christian Counseling Certification
Now I do not mean to dismiss the haste in which Ignatius says a soul can lose friendship with God through mortal sin, but the act of mortal sin as an objective act and its consequences upon the subjective agent can be quite differently applied. There are many souls who share sins committed on earth who are in Heaven as those who are in Hell. The difference is contrition but also charity. A soul that occasionally falls into certain sins that are classified as mortal, such as many sexual sins, does face severe danger than mere minor sins, but again all sin separates the soul from God to some degree and how the soul responds to hurting God via love matters. A soul that goes to Hell obviously exists in Mortal sin at the time of death. Obviously, these sins have defined the soul’s character and sealed its fate. Whether they were sexual sins, or sins of murder, rape, or even cases of extreme self love and unkindness to others and complete worship of this world over God, these sins represent a pattern. There are some sins especially among the deadly that represent a median line that show a point of no return or least hint towards it. Despite this, all can be converted and changed while alive, one merely needs to look at the story of St Augustine or even St Paul, but when a serious sin becomes more than an “oops” and “mistake” but enters into a habitual state of sin that renounces God and exalts self then a serious condition of darkness envelops the soul. Unlike the angels, the human intellect cannot make a decisive decision regarding to love or serve God, instead over time, the soul develops into what it will be. Hence eventually, a soul can cross a line that has led to a serious life threatening level that if one dies in it, will result in Hell. There are death bed conversions, but when one examines the life of Hitler, Stalin, or even pedofiles and sex traffickers or those consumed by lust and the sexual industry, one can see a strong difference in the deformation of the soul between one who occasionally yet with regret fell into a few serious sins as opposed to those who lived in it all the time and became committed it to the most extreme levels.
The biggest difference for the soul that chooses Hell is one that not only commits serious sin, but accepts it, loves it and live in it. I do not wish to dismiss the frightful examples of Ignatius in his exercises of one un-repented mortal sin, but I think if one understands moral theology, the psychology of the soul, as well habit in life, one is more likely to discover that most souls who go to Hell, choose it freely and not by accidentally and remorsefully tasting sin here and there. Those with broken natures who fall into serious sin as lost children can indeed if absence of remorse can find their soul in rebellion to God, but most who have conscience, who love God despite failings, rarely allow the life style to infect themselves. Instead they turn to prayer, humility and remorse. The soul that chooses Hell loves oneself over God. The soul in Hell has no charity for others. The soul in Hell sees no wrong in its actions. The soul in Hell lived in sin and embraced it. The soul in Hell does not love God, nor His laws. The soul in Hell, whether consciously or subconsciously, committed these actions with pure love and habitual opportunity without remorse. They were not merely serious sexual or selfish sins of occasion or weakness of moment, but conscious and autonomous choices of life. There was an autonomous intent and a complete disclosure in the choices it made.
These souls at the Partial Judgement are stripped of their distractions or excuses and left with the cold verdict of God. The verdict is a lack charity or love of God or others but instead complete love of self and the world. God’s verdict and justice is declared but His mercy still extends to these individuals. This may seem surprising but God still reaches out to those who even reject His love. God is still willing to forgive, but the judgement of His perfect and true self shines so brightly that such a broken and disordered soul cannot disagree with its own deformation and mutation. The soul going to Hell knows what it is and through this mirror and judgement openly rejects the mercy that comes with the justice. So, in a complete truthful image, God does judge, but God also grants mercy. In way, God’s justice does send the soul to Hell, but it is in a far different way than one’s human sense imagines it. The soul going to Hell instead rejects God and His assessment and mercy. It rejects consequences or needed remorse. It rejects even God’s mercy. This self inflicted wound is a continuation of the habitual sinful choices during life on earth that sends the soul to Hell.
On the contrary, a soul that is both saint and sinner, reflects on its image and is brought to shame and guilt but still expresses love. This soul did not die void of grace that serious sin strips from the soul but it died with grace and its most important fruit which is love. Whether more perfectly or less perfectly, a person’s love for God travels with person before the judgement of God. This love of God over love of self is the starting point of salvation for that soul. Again whether a great saint or a pitiful sinner who still finds love of God, neither are worthy of Heaven based on their individual merit due to one’s broken nature. It is solely the grace earned by Christ and one’s cooperation throughout life with grace that permits anyone to enter into union with God. The graces that energized faith and hope now fade because faith and hope have delivered what was promised. As Scripture foretells, what then remains is love. If love remains in a soul, then that soul remains in the state of grace. This soul tried its best to avoid sin, as well as serious sin, and when it fell, it humbly sought forgiveness and purged itself with tears and penance. Unlike the soul that chose Hell by its continual choices on earth, the same soul that chose Heaven chose God for most of its life and at the very end. Despite its sins, despites its failures, God and the saved soul share a reciprocal love that manifests acceptance of God’s love and will. The soul then understands clearly that it may not have loved God as much as it needed on earth but God’s love and grace has sanctified it and made it worthy.
Conclusion
Please also review AIHCP’s Christian Counseling Certification
When exploring the judgement of God and his justice and mercy, the motifs of God as judge, are applicable, and true. God is just. However, He is also merciful. He is both the God of justice but also the God of mercy as the Prodigal Son illustrated in Christ’s parable. God understands human beings are broken despite His Son’s death on the cross. He is patient, He is loving and waits for His sheep like the Good Shepherd. He does not despise the wicked but rejects their actions. He judges them based on their own deeds and decisions in life. He offers justice but also offers mercy. Ultimately, the soul dictates its future. I think it is important pending on the season or need to review both God’s justice and mercy. Ignatius will presenting a merciful God, also presents a terrifying view of judgement, Hell and the nature of sin. In addition balance this with Padre Pio’s teaching on the choice of Hell being usually more so a life time choice over time and self love and to be aware of how sin breaks us down over time. We still must be alert of individual sin in the moment, but we must remain strong and steadfast to identify it and repent from it. Sister Faustina’s Divine Mercy also displays Christ’s great love and mercy that one can find. So balance in understanding God’s mercy but also justice can help one remain steadfast in confidence of God’s love but also our own important role in keeping the commandments.
In closing, f anyone is a parent, then one understands the deep love one has a for one’s child or children. One never gives up on a child and loves the child even when the child does wrong. When the child does not seek reconciliation, it painfully hurts. Even when they walk away, the hand still extends for the child who never looks back again. While God in Scripture is seen as judge and rightfully so, it is important to see God also as a parent. Unlike some of the more vivid meditations of St Ignatius, God’s judgement does cast those to Hell but not maybe the way one envisions it, but more so as a parent who displays what must be obeyed if one chooses to return and the consequences hereafter. If the child shows just the bit of love, God, like a parent, can capitalize on that but if the child shows no love or desire to obey, and chooses instead to reject the parent, then based off his analogy, God can only watch the person enter into Hell. The terrifying reality that one sends oneself to Hell. So remain vigilant to sin, but most importantly avoid serious sin. If one falls, allow one’s conscience to identify and seek repentance. Sin is deadly and builds upon the soul and hopes to turn one serious event into continuous a life style. Maintain charity and love of God with remorse. If so, when one stands before God, it will not be a strange judge, but a loving parent.
AIHCP has numerous blogs based on Carl Rogers and his Client or Human/Person Centered Based Counseling. This blog will focus some on the general themes, goals and history of the therapy and how it set the standard for many modern day counseling techniques. Whether one belongs solely to Rogerian Counseling, or instead mixes and matches some of the philosophies and skills where needed, it remains nearly impossible for numerous Rogerian ideals not to be part of any counseling curriculum and utilized within the professional and clinical spectrum.
Please also review AIHCP’s various Behavioral and Healthcare Certifications and see if they meet your academic and professional goals.
Rogerian Psychology and Counseling- A Client/Person Centered Approach
Rogerian or person centered counseling finds its roots in counselors who express empathy and unconditional positive regard
In essence, Rogers possessed a more optimistic account of human nature and believed that helping people involved helping them help themselves and find inner healing. Instead of diagnosis, or pre-determined psycho-analysis, Roger developed a psychology and counseling that frowned upon diagnosis as well as counselor authoritarian directives but saw the counselor more as a guide and helper in unlocking a person’s potential to find happiness and balance in life. This type of counseling took some key core concepts from Adler and then became a main stay in the counseling fields since the Mid 20th Century.
Rogers taught that counselors need to help clients self-actualize to become their best self. This was accomplished through guidance that helped the person choose what is best for them. The counselor could help a person reach self actualization by helping them find congruence or genuineness with their true self. When a person was at odds with their true self or their words did not match their deeds, a counselor could help a person see this incongruence (Tan, 2022). In addition to helping a person actualize self, counselors within Rogerian schools of thought help clients understand the value of their own subjective experiences. Rogers believed that the subjective experience of a person was the most true form of self and the best way to find congruence within a person. However, the most lasting and important aspect involves the client’s condition of worth. Rogers emphasized that counselors must show deep empathy, unconditional positive regard and genuineness as core concepts in helping people (Tan, 2022). Ultimately the basis of Rogerian therapy is to not solve problems but to unlock an individual’s own solving problem abilities (Tan, 2022).
In other blogs, we discuss the critical importance of unconditional positive regard, congruence and empathy. These again are the most lasing elements of Rogerian psychology. While many adhere to some of the other concepts of subjective experience, or the role of the counselor, these three standards of counseling remain core in most counseling schools as essential elements in helping people. Beyond just being taught, these lasting qualities of the counselor also show empirically and in clinical studies strong effectiveness in helping the client. While classic Rogerian counseling swayed away from diagnosis or various therapeutic strategies, it always emphasized the importance of the counselor/client relationship. In many studies, this is the most key part whether counseling works or not. While various therapeutic strategies are essential, which ones used or not used, has more power when amplified with the counselor/client relationship.
In recent years, Rogerian Counseling has also been transformed by modifications, such Motivational Interviewing. Tan points out that this is also a person centered approach and also has many shared core elements (2022). Initially developed by William Miller, Motivational Interviewing utilizes Rogerian strategies and counselor based qualities to help clients reach goals. Tan points out that Motivational Interviewing is a collaborative approach of strengthening a person’s motivation and commitment to change. He also points out that it looks to address the ambivalence about change and is designed to help the person’s motivation by assigning goals and also exploring a person’s reasons to look for change (2022).
Interviewing involves utilizing empathy, congruence as well as unconditional positive regard, but also involves the counselor rolling with resistance of the client in a non-confrontational way. Instead helping to facilitate a picture for the client to see on one’s own to desire the change. In doing so, the counselor helps to support self efficacy and freedom of choice to fully embrace a change and work towards a goal (Tan, 2022).
Strengths and Weaknesses
Like any counseling system or psychological school of thought, one can be tied down and limited if only subject to one way of doing things with the psychological mind. This bears true with one who only utilizes psychodynamic ways without integration of other possible therapies in the cognitive fields, or for that matter approaching one from a cognitive or behavioral school of thought. Like wise, person centered psychology and counseling has strengths that can be employed, but also weaknesses when isolated and used as a the only way conducting counseling.
From a strength standpoint, the utilization of the concepts of unconditional positive regard, congruence and empathy are all staples of modern counseling. Person centered therapy also has a very optimistic view of a the human person and is rich in encouraging and helping someone find the ability to change through one’s innate abilities. It treasures freedom to choose which is the only way true change can occur.
From a weakness standpoint, it ins purest form, it avoids diagnosis and some therapies which when involving deeper trauma or pathology require more than just discussing an issue but also helping the mind heal through other proven strategies. Also, it emphasizes a complete subjective form of happiness and process of making decisions. This can lead to one’s own selfish motives, as well as choosing incorrectly in the overall scheme of life. Counselors while observing need to sometimes direct. Rogers did point to empathetic confrontation, but it needs to sometimes go farther than merely helping a person see the contradiction in one’s life but to also sometimes guide the person to the right choice. In Rogerian psychology, the counselor remains as benign a source of authority as possible in regards to direction. Many clients need guidance. This is not to assert they need told what and how to do something, but sometimes, a person needs direction. The concepts of subjective truth also come into conflict with many ideals on objective truth, as well as the person belonging to more than merely oneself but also belonging to a social construct that includes other people, as well as religious beliefs. For some, God is the source of self actualization, not the human person. For others, self actualization can become a very selfish design that ignores others and their needs. (Tan, 2022).
So again, I feel there always needs to be a measure of balance with any systems of psychology and counseling. While schools of thought exist in their purity, many counselors utilize the best of all the schools and fit it to meet the unique needs of a client.
Conclusion
Please also review AIHCP’s Healthcare Certification programs and see if they match your academic or professional goals
Carl Rogers ideas and philosophies presented to counseling were revolutionary when compared to Freudian systems. It expressed that individuals were not preprogrammed and had the innate ability to find congruence when guided by a trained counselor. The counselor was not there to solve problems but help untap the ability of the client to solve their problems. This leads to a very subjective experience of self actualization which has its strengths and weaknesses in counseling. The largest contribution of Rogers was the counseling qualities he demanded from all counselors. Namely congruence, empathy and unconditional positive regard. These elements help forge a healthy counselor and client relationship which according to studies is more important and a bigger factor in client progress than any particular therapeutic strategy employed alone. It is the counselor and client’s relationship that is the biggest factor in whether the counseling experiment works or does not work.
Please also review AIHCP’s Behavioral Health Certifications in Grief Counseling, Christian Counseling, Trauma Counseling, Crisis Counseling, Stress Management and Anger Mangement.












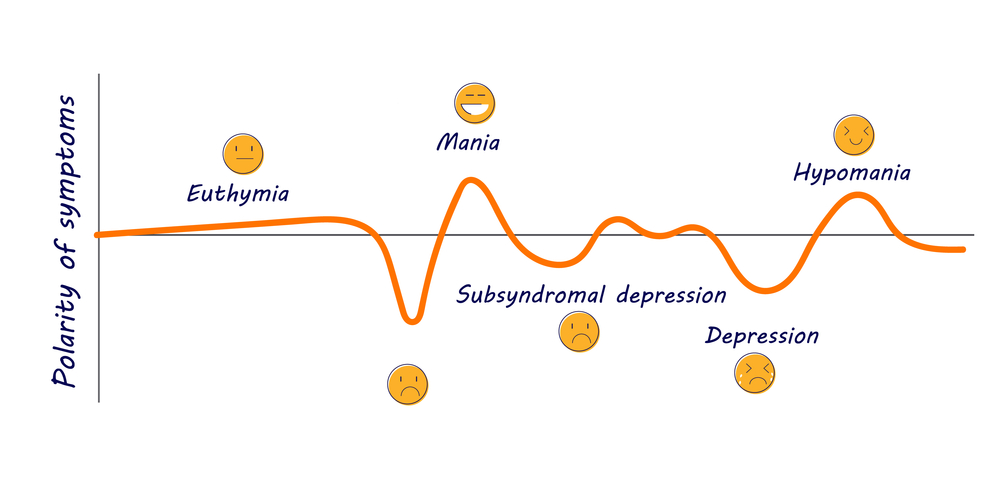











 Written by
Written by