Mood disorders transcend the usual care of pastoral or non-clinical grief counselors. Most grief counselors deal with the natural phenomena of loss that follows a natural grief trajectory. Clinical professionals, who may also be grief counseling certified, deal with pathological issues surrounding mood. Any instability of extremes, whether due to mania or melancholy can disrupt natural life and harm mental health. Sometimes, moods can be directly affected by an acute grief or loss and this leads down a trajectory of complications due to grief, while in other cases, there is no triggering loss that causes the pathological mood. Instead it involves an in-depth investigation into the etiology of the disorder reviewing biological, genetic, psychological, social and spiritual issues to explain the condition.
The DSM-V-TR groups together a variety of mood disorders which in this blog will highlight Major Depressive Disorder, Persistent Depressive Disorder and its numerous specifiers, as well as Bi-Polar 1 and Bi Polar 2 disorders and finally, Prolonged Grief Disorder. It is important to remember that for the pastoral or non-clinical grief counselor, one should have a strong understanding of these mood disorders to help refer clients to the appropriate clinical specialists. A non-clinical grief counselor cannot diagnose or treat mood disorders but they can be trained to spot these disorders and work with clinical professionals in assuring the necessary therapy and medications are received for the client.
Please also review AIHCP’s Grief Counseling Certification, as well as its numerous other Grief Programs.
Etiology of Mood Disorders
Mood disorders find their etiology from numerous factors. Biologically, whether mania or melancholic, there is a strong connection of genetic inheritance of these pathologies tied to the neurotransmitters (McRay,2016). When the neurotransmitter, serotonin, is low, depressive states can exist. Serotonin is the a critically important neurotransmitter for mood stability (Barlow, et. al., 2023). In regards to mania, the synapses between neurons fire to fast, and a euphoric state overtakes the person. This is usually due to higher levels of the neurotransmitter norepinephrine and lower of levels of serotonin, although higher levels of serotonin can also lead to states of mania (McRay, 2016).
Depression can be caused by an internal trigger but also a stressor or external loss. Hence unipolar mood disorders can be both have a direct external stimuli as well as an internal disruption. Many times the diathesis or culmination of internal and external events that overcomes a person to the disorder can be attributed to external factors that activate it. As similar to anxiety disorders, a loss, or lack of social support in that loss, or distorted cognitive thinking can unravel a person’s natural reactions into a pathological state (Barlow, et. al. 2023).
When considering psychological etiology for mood disorders, many aspects involve self image, cognitive distortions, as well as learned helplessness in situations. When individuals engage in self negative talk and think the worst, then it can affect a person’s overall mental paradigm. In addition, when a person feels they have no control or power to prevent bad things from continuing, then the person becomes susceptible to pathological mood disorders (McRay, 2016). In addition to how one thinks, social and cultural and spiritual aspects play a key role. A person’s support system is key in any mood stabilization because it determines the foundation one has to face multiple problems before succumbing to the issue. In addition, culturally and spiritually, how one views loss can play a key role in how one reacts to loss.
As one can see, mood disorders are a complications of genetic but also psychological, social, cultural and spiritual aspects of the person. Sometimes, the mood disorder, such as depression, has a visible trigger, but other times, it is purely at the chemical level of the brain. Every individual is different and what causes diathesis and activation of a mood disorder, or even anxiety is not a simple equation but a very complex one.
Mood Disorders and the DSM-V-TR
In this blog, we will follow the order of the DSM-V-TR and how it lists and discusses the nature of mood disorders. We will primarily focus only on the above mentioned disorders.
Bi Polar I & Bi Polar II Disorder
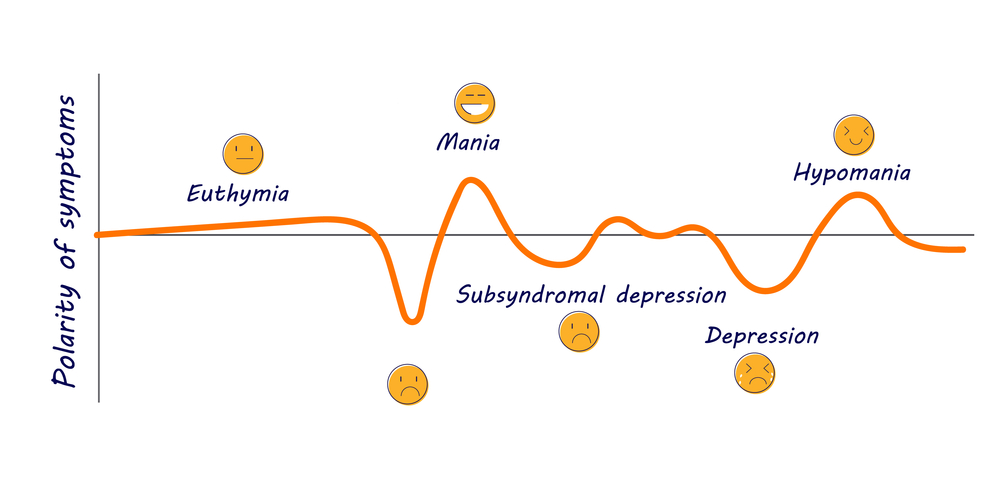
Bi polar disorders are characterized by cycles of depression and euphoria (mania) with symptoms that can greatly affect one’s ability to function in life (McRay, 2016). The DSM-V-TR states that mania is a period of abnormal and persistent moods of high levels of energy with the possibility of also irritability which lasts at least 1 week (2022). During this phase of mania, the DSM-V-TR notes these types of characteristics with three needed for diagnosis or four if the mood is only irritability.
- inflated self esteem or grandiosity
- deceased need for sleep
- more talkative or need to talk
- flights of ideas or subjective experiences that are racing through the mind
- distractibility
- increased goal directive activities that can be social, work, academic or sexually
- excessive engagement in activities with high potential for bad outcomes. Such as foolish business investments, spending sprees or sexual activitiy
The DSM-V-TR continues that these states cause severe impairment to social and occupational functioning and has no association with other psychotic, psychological, substance or medicated purposes (2022). Within itself, these are conditions for mania, which albeit rare, can exist as an issue alone apart from Bi-Polar I or II.
Ironically, Bi-Polar I does not require a depressive cycle although that is very rare for one not to be present in diagnosis. When we discuss Major Depressive Disorder and a depressive episode we will list its diagnosis as well which would be utilized with any Bi-Polar disorder.
For Bi-Polar I, as well as Bi-Polar II, the DSM-V-TR provides many specifiers since it affects individuals with so many additional subjective aspects. It can be mild, moderate, severe, possess psychotic features, be in partial remission or full remission, or also include anxious distress, mixed features, rapid cycling, melancholic features, mood congruent psychotic features or mood incongruent psychotic features, catonia, peripartum or seasonal (2022).
Bi-Polar II differs from Bi- Polar I in that there is no state of mania but there always must be a depressive state. What replaces mania is referred to hypomania. Hypomanic episodes shares the same characteristics of mania but not as severe or impairing to the individual (only 4 days as opposed to at least a week) but it still manifests a change in functioning that is not characteristic of the individual when not symptomatic (2022). In addition, the mood shift is observable by others but not enough to cause extreme distress (DSM-V-TR, 2022).
The primary differing diagnosis factor from Bi-Polar I over Bi-polar II is one has not ever been diagnosed with a true mania state ever in life.
It is important to note, some individuals who suffer from Bi-Polar mood disorders cycle more rapidly than others, with 4 mood shifts a year being considered high but there can be less cycles and individuals can move through them quickly (Barlow, et. al, 2023).
Major Depressive Disorder
While depressive episodes are part of bipolar disorders, the same criteria for Major Depressive Disorder that diagnoses an episode of depression for Bi-Polar disorders is also diagnosis Major Depressive Disorder but without any mania or states of euphoria. Major Depressive Order can find its origins biologically or also be a reaction to a loss or severe stressor. It is a unipolar mood disorder without a switching from extremes but a state of melachony
According to the DSM-V-TR depressed moods or loss of interest in pleasure must persist for periods of 2 weeks or longer (2022). Diagnostic characteristics include the following and requires five or more symptoms for diagnosis.
- Depressed mood for most of the day or nearly everyday. Feelings of sadness, emptiness and hopelessness
- Diminished interest in pleasure
- significant weight loss
- Insomnia or hypersomnia nearly or everyday
- psychomotor agitation that is observable by others
- fatigue and lack of energy nearly everyday
- feelings of guilt or unworthiness
- diminished ability to concentrate or think or make decisions
- recurrent thoughts about death, recurrent suicidal ideation without a specific plan or with a plan, as well as suicide attempt
These symptoms impair the individual in all aspects of life and are not due to any other psychological, medical or use of substance (2022).
Like bi-polar mood disorders, Major Depressive Disorder also has specifiers that dictate mild, moderate, severe, with psychotic features, partial or full remission, with anxious distress, mixed features, melancholic features, atypical features, mood congruent or mood incongruent psychotic features, catonia, post partem, or seasonal patterns (SAD) (DSM-V-TR, 2022).
Overall, Major Depressive Disorder is one of the most common mental maladies. It is considered the common cold of mental health (McRay, 2016). Women are 2 to 1 more likely to develop it, while Bi-Polar Disorder is equal (McRay, 2016).
Mentally, an individual suffering from depression faces the depressive cognitive triad that perceives negative connotations about self, the world and the future (Barlow, et. al., 2023).
Persistent Depressive Disorder
Persistent Depressive Disorder differs from Major Depressive Disorder in that is lasts longer than the normal minimum of 2 weeks but untreated can persist for months to years to decades. It is not as intense but it leads to numerous health and mental issues. Diagnosis requires a consistent 2 year period. It includes poor appetite or overeating, insomnia or hyperinsomnia, low energy, low self-esteem, poor concentration and feelings of hopelessness, (DSM-V-TR, 20220). Individuals can also suffer from both Persistent and Major Depressive.
Other Mood Disorders
Other mood disorders include Disruptive Mood Dysregulation Disorders that deal with frustration and anger outbursts, as well as Cyclothymic Disorder which does not meet criteria for mania, hypnomania or depressive episodes but still possess similar traits at a less severe level but for a period of 2 years with impaiment.
Ironically, Prolonged Grief Disorder is not associated with mood disorders in the DSM-V-TR but is a stress related disorder to acute grief which resembles depression but is a complex grief reaction. The trajectory of normal reaction to loss is distorted due to severity of the loss, or various subjective factors involving the person. AIHCP has numerous blogs on Complicated Grief as well as Prolonged Grief Disorder.
Treatments for Mood Disorders
Treatment for mood disorders should also include a integrated approach that includes medication as well as therapy. Medication only masks the problem and without life skills and abilities to understand distorted thinking, then long term healing and mental health is not possible. Also, some medications have complications which involves alternate trials and errors of different medications. In addition, many individuals feel a mental stigma when diagnosed with depression or bipolar disorders. This leads to hiding these feelings, or refusing to take the appropriate medications. This leads to continued chaos, impairment, broken relationships, loss careers, and wasted time. It is important to face mood disorders as any health condition.

Medications
Anti-depressants are utilized to help most individuals with mood disorders, especially melancholy. There are three types. First, SSRIs are the most common and most used in modern medicine. Second, tricyclic and third, monamine oxidase (MAO). The tricyclics are rarely used with the advent of SSRI’s since tricyclics had more side effects. SSRI’s stand for Selective Serotonin Reuptake Inhibitor. They prevent the transfer of serotonin from one neuron to another hence preserving a higher level of serotonin to the body to help maintain mood. MAO’s help dissolve the break down of Serotonin (Barlow, et. al., 2023). Barlow notates that 60 to 70 percent of individuals who take medication for depression experience improvement, with half of that meeting full to close recovery to full functioning (2023). A common SSRI’s include Prozac (fluoxetine). Others include Celexa, Lexapro, Luvox, Paxil and Zoloft. Sometimes, individuals must go through a regiment of different SSRI until they find the best fit and dosage necessary to manage the depression. Some need to be on SSRI longer, while others are dosed and gradually let off as needed.
Those who face treatment resistant depression can also turn to other methods to treat depression. Holistic and natural remedies under the guidance of a primary physician such as St. John’s Wort or hypericum have shown benefits as well (Barlow, et. al., 2023). Other more direct methods include Transcranial Magnetic Therapy (TMT) as well as Electroconvulsive Therapy (ECT) which directly sends impulses into the brain and neurons (Barlow, et al., 2023).
In regards to bi-polar disorders, a lithium based medication is utilized to help with mania. Lithium, a common salt in the natural environment, needs to be carefully dosed but has success with controlling mania states. It is associated with weight gain which is another reason many individuals with bi-polar disorders wish to avoid their medication (Barlow, et. al., 2023).
Psychotherapy
Psychotherapy when supplemented with medication is the best combo for treating mood disorders. It is important to fix the chemical issue but one also needs to have a strong understanding of self and ways to think differently. Cognitive Behavioral Therapy plays a key role in helping individuals reframe and rethink distortions and negative connotations about self. An individual who is depressed already has negative connotations about self, the world and the future. AIHCP has blogs about CBT and its importance as a behaviorist therapy stemming from Aaron Beck and Albert Ellis that looks to help individuals think more healthy for better behavior and mental functioning. In addition, human centered therapies which gravitate towards self esteem and congruence and fulfillment are important. Karl Rogers and his person-centered therapy looks to support the client in meeting fulfillment through empathy, genuineness and unconditional positive regard. AIHCP also has a blog to review on human-centered therapies. Finally, interpersonal skills and support is key. Individuals suffering from loss need support. An individual with better support systems can overcome different losses with more success. Some have stronger internal systems of meaning and spirituality, while others may have more family or friends or financial means to overcome loss. Basic grief counseling in these ways can help individuals become more resilient when depressed or sad.
Conclusion

Mood disorders can be stable with only one extreme or unstable and shift from mania to melancholy. They are among, with anxiety, the most common psychopathologies. Unfortunately, many individuals avoid treatment due to social stigma. It is important to find the time to take care of one’s mental health if afflicted with a mood disorder. Mood disorders can be genetic or causal but most all have solutions via medication, psychotherapy and counseling, or an integrated approach.
Please also review AIHCP’s Grief Counseling Certification as well as AIHCP’s multiple other behavioral health certification programs.
Additional Blogs
Anxiety Disorders: Access here
Grief Video: Grief: The Price of Love. Access here
Additional Resources
Bipolar Disorder. Mayo Clinic. Access here
Clinical Depression (Major Depressive Disorder). (2026). Cleveland Clinic. Access here
Dimaria, L. (2026). “Types of Mood Disorders”. VeryWellMind. Access here
References
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorder” DSM-5-TR (5th ed., text revision). American Psychiatric Association Publishing.
Barlow, D.H., Durand, V.M., & Hofmann, S.G. (2023). Psychopathology. An integrative approach to mental disorder (9th ed.). Cengage Learning
McRay, B.W., Yarhouse, M.A., Butman, R.E., & Kiple, C. (2016). Modern psychopathologies: A comprehensive Christian appraisal. (2nd, ed.) IVP Academic
 Written by
Written by 


 Written by Marko,
Written by Marko,