Mood disorders transcend the usual care of pastoral or non-clinical grief counselors. Most grief counselors deal with the natural phenomena of loss that follows a natural grief trajectory. Clinical professionals, who may also be grief counseling certified, deal with pathological issues surrounding mood. Any instability of extremes, whether due to mania or melancholy can disrupt natural life and harm mental health. Sometimes, moods can be directly affected by an acute grief or loss and this leads down a trajectory of complications due to grief, while in other cases, there is no triggering loss that causes the pathological mood. Instead it involves an in-depth investigation into the etiology of the disorder reviewing biological, genetic, psychological, social and spiritual issues to explain the condition.
The DSM-V-TR lists numerous mood disorders ranging from Major Depressive Disorder to Bi-Polar Disorders. Please also review AIHCP’s Grief Counseling Certification
The DSM-V-TR groups together a variety of mood disorders which in this blog will highlight Major Depressive Disorder, Persistent Depressive Disorder and its numerous specifiers, as well as Bi-Polar 1 and Bi Polar 2 disorders and finally, Prolonged Grief Disorder. It is important to remember that for the pastoral or non-clinical grief counselor, one should have a strong understanding of these mood disorders to help refer clients to the appropriate clinical specialists. A non-clinical grief counselor cannot diagnose or treat mood disorders but they can be trained to spot these disorders and work with clinical professionals in assuring the necessary therapy and medications are received for the client.
Mood disorders find their etiology from numerous factors. Biologically, whether mania or melancholic, there is a strong connection of genetic inheritance of these pathologies tied to the neurotransmitters (McRay,2016). When the neurotransmitter, serotonin, is low, depressive states can exist. Serotonin is the a critically important neurotransmitter for mood stability (Barlow, et. al., 2023). In regards to mania, the synapses between neurons fire to fast, and a euphoric state overtakes the person. This is usually due to higher levels of the neurotransmitter norepinephrine and lower of levels of serotonin, although higher levels of serotonin can also lead to states of mania (McRay, 2016).
Depression can be caused by an internal trigger but also a stressor or external loss. Hence unipolar mood disorders can be both have a direct external stimuli as well as an internal disruption. Many times the diathesis or culmination of internal and external events that overcomes a person to the disorder can be attributed to external factors that activate it. As similar to anxiety disorders, a loss, or lack of social support in that loss, or distorted cognitive thinking can unravel a person’s natural reactions into a pathological state (Barlow, et. al. 2023).
When considering psychological etiology for mood disorders, many aspects involve self image, cognitive distortions, as well as learned helplessness in situations. When individuals engage in self negative talk and think the worst, then it can affect a person’s overall mental paradigm. In addition, when a person feels they have no control or power to prevent bad things from continuing, then the person becomes susceptible to pathological mood disorders (McRay, 2016). In addition to how one thinks, social and cultural and spiritual aspects play a key role. A person’s support system is key in any mood stabilization because it determines the foundation one has to face multiple problems before succumbing to the issue. In addition, culturally and spiritually, how one views loss can play a key role in how one reacts to loss.
As one can see, mood disorders are a complications of genetic but also psychological, social, cultural and spiritual aspects of the person. Sometimes, the mood disorder, such as depression, has a visible trigger, but other times, it is purely at the chemical level of the brain. Every individual is different and what causes diathesis and activation of a mood disorder, or even anxiety is not a simple equation but a very complex one.
Mood Disorders and the DSM-V-TR
In this blog, we will follow the order of the DSM-V-TR and how it lists and discusses the nature of mood disorders. We will primarily focus only on the above mentioned disorders.
Bi Polar I & Bi Polar II Disorder
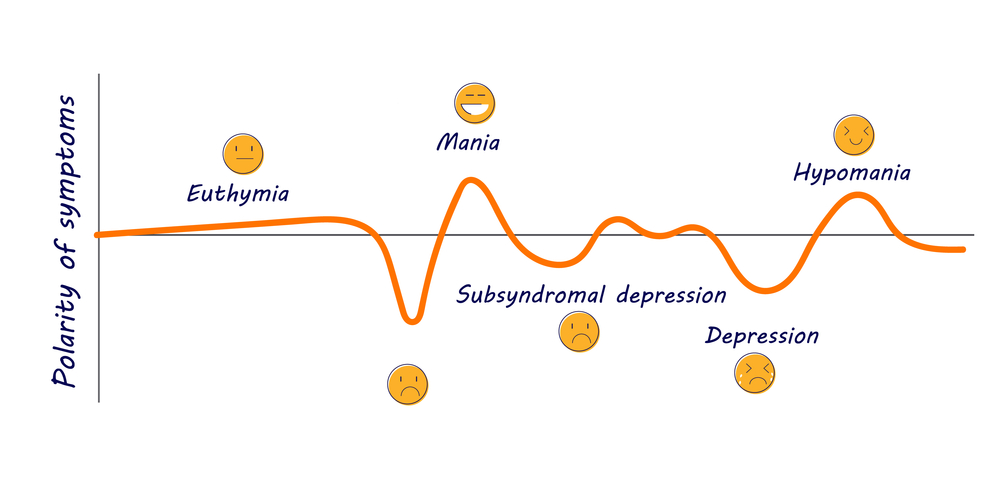
Polarity of symptoms Depression euthymia mania subsyndromal hypomania. Vector illustration
Bi polar disorders are characterized by cycles of depression and euphoria (mania) with symptoms that can greatly affect one’s ability to function in life (McRay, 2016). The DSM-V-TR states that mania is a period of abnormal and persistent moods of high levels of energy with the possibility of also irritability which lasts at least 1 week (2022). During this phase of mania, the DSM-V-TR notes these types of characteristics with three needed for diagnosis or four if the mood is only irritability.
inflated self esteem or grandiosity
deceased need for sleep
more talkative or need to talk
flights of ideas or subjective experiences that are racing through the mind
distractibility
increased goal directive activities that can be social, work, academic or sexually
excessive engagement in activities with high potential for bad outcomes. Such as foolish business investments, spending sprees or sexual activitiy
The DSM-V-TR continues that these states cause severe impairment to social and occupational functioning and has no association with other psychotic, psychological, substance or medicated purposes (2022). Within itself, these are conditions for mania, which albeit rare, can exist as an issue alone apart from Bi-Polar I or II.
Ironically, Bi-Polar I does not require a depressive cycle although that is very rare for one not to be present in diagnosis. When we discuss Major Depressive Disorder and a depressive episode we will list its diagnosis as well which would be utilized with any Bi-Polar disorder.
For Bi-Polar I, as well as Bi-Polar II, the DSM-V-TR provides many specifiers since it affects individuals with so many additional subjective aspects. It can be mild, moderate, severe, possess psychotic features, be in partial remission or full remission, or also include anxious distress, mixed features, rapid cycling, melancholic features, mood congruent psychotic features or mood incongruent psychotic features, catonia, peripartum or seasonal (2022).
Bi-Polar II differs from Bi- Polar I in that there is no state of mania but there always must be a depressive state. What replaces mania is referred to hypomania. Hypomanic episodes shares the same characteristics of mania but not as severe or impairing to the individual (only 4 days as opposed to at least a week) but it still manifests a change in functioning that is not characteristic of the individual when not symptomatic (2022). In addition, the mood shift is observable by others but not enough to cause extreme distress (DSM-V-TR, 2022).
The primary differing diagnosis factor from Bi-Polar I over Bi-polar II is one has not ever been diagnosed with a true mania state ever in life.
It is important to note, some individuals who suffer from Bi-Polar mood disorders cycle more rapidly than others, with 4 mood shifts a year being considered high but there can be less cycles and individuals can move through them quickly (Barlow, et. al, 2023).
Major Depressive Disorder
While depressive episodes are part of bipolar disorders, the same criteria for Major Depressive Disorder that diagnoses an episode of depression for Bi-Polar disorders is also diagnosis Major Depressive Disorder but without any mania or states of euphoria. Major Depressive Order can find its origins biologically or also be a reaction to a loss or severe stressor. It is a unipolar mood disorder without a switching from extremes but a state of melachony
Facing Major Depressive Disorder
According to the DSM-V-TR depressed moods or loss of interest in pleasure must persist for periods of 2 weeks or longer (2022). Diagnostic characteristics include the following and requires five or more symptoms for diagnosis.
Depressed mood for most of the day or nearly everyday. Feelings of sadness, emptiness and hopelessness
Diminished interest in pleasure
significant weight loss
Insomnia or hypersomnia nearly or everyday
psychomotor agitation that is observable by others
fatigue and lack of energy nearly everyday
feelings of guilt or unworthiness
diminished ability to concentrate or think or make decisions
recurrent thoughts about death, recurrent suicidal ideation without a specific plan or with a plan, as well as suicide attempt
These symptoms impair the individual in all aspects of life and are not due to any other psychological, medical or use of substance (2022).
Like bi-polar mood disorders, Major Depressive Disorder also has specifiers that dictate mild, moderate, severe, with psychotic features, partial or full remission, with anxious distress, mixed features, melancholic features, atypical features, mood congruent or mood incongruent psychotic features, catonia, post partem, or seasonal patterns (SAD) (DSM-V-TR, 2022).
Overall, Major Depressive Disorder is one of the most common mental maladies. It is considered the common cold of mental health (McRay, 2016). Women are 2 to 1 more likely to develop it, while Bi-Polar Disorder is equal (McRay, 2016).
Mentally, an individual suffering from depression faces the depressive cognitive triad that perceives negative connotations about self, the world and the future (Barlow, et. al., 2023).
Persistent Depressive Disorder
Persistent Depressive Disorder differs from Major Depressive Disorder in that is lasts longer than the normal minimum of 2 weeks but untreated can persist for months to years to decades. It is not as intense but it leads to numerous health and mental issues. Diagnosis requires a consistent 2 year period. It includes poor appetite or overeating, insomnia or hyperinsomnia, low energy, low self-esteem, poor concentration and feelings of hopelessness, (DSM-V-TR, 20220). Individuals can also suffer from both Persistent and Major Depressive.
Other Mood Disorders
Other mood disorders include Disruptive Mood Dysregulation Disorders that deal with frustration and anger outbursts, as well as Cyclothymic Disorder which does not meet criteria for mania, hypnomania or depressive episodes but still possess similar traits at a less severe level but for a period of 2 years with impaiment.
Ironically, Prolonged Grief Disorder is not associated with mood disorders in the DSM-V-TR but is a stress related disorder to acute grief which resembles depression but is a complex grief reaction. The trajectory of normal reaction to loss is distorted due to severity of the loss, or various subjective factors involving the person. AIHCP has numerous blogs on Complicated Grief as well as Prolonged Grief Disorder.
Treatments for Mood Disorders
Treatment for mood disorders should also include a integrated approach that includes medication as well as therapy. Medication only masks the problem and without life skills and abilities to understand distorted thinking, then long term healing and mental health is not possible. Also, some medications have complications which involves alternate trials and errors of different medications. In addition, many individuals feel a mental stigma when diagnosed with depression or bipolar disorders. This leads to hiding these feelings, or refusing to take the appropriate medications. This leads to continued chaos, impairment, broken relationships, loss careers, and wasted time. It is important to face mood disorders as any health condition.
SSRI help stabilize serotonin and mood
Medications
Anti-depressants are utilized to help most individuals with mood disorders, especially melancholy. There are three types. First, SSRIs are the most common and most used in modern medicine. Second, tricyclic and third, monamine oxidase (MAO). The tricyclics are rarely used with the advent of SSRI’s since tricyclics had more side effects. SSRI’s stand for Selective Serotonin Reuptake Inhibitor. They prevent the transfer of serotonin from one neuron to another hence preserving a higher level of serotonin to the body to help maintain mood. MAO’s help dissolve the break down of Serotonin (Barlow, et. al., 2023). Barlow notates that 60 to 70 percent of individuals who take medication for depression experience improvement, with half of that meeting full to close recovery to full functioning (2023). A common SSRI’s include Prozac (fluoxetine). Others include Celexa, Lexapro, Luvox, Paxil and Zoloft. Sometimes, individuals must go through a regiment of different SSRI until they find the best fit and dosage necessary to manage the depression. Some need to be on SSRI longer, while others are dosed and gradually let off as needed.
Those who face treatment resistant depression can also turn to other methods to treat depression. Holistic and natural remedies under the guidance of a primary physician such as St. John’s Wort or hypericum have shown benefits as well (Barlow, et. al., 2023). Other more direct methods include Transcranial Magnetic Therapy (TMT) as well as Electroconvulsive Therapy (ECT) which directly sends impulses into the brain and neurons (Barlow, et al., 2023).
In regards to bi-polar disorders, a lithium based medication is utilized to help with mania. Lithium, a common salt in the natural environment, needs to be carefully dosed but has success with controlling mania states. It is associated with weight gain which is another reason many individuals with bi-polar disorders wish to avoid their medication (Barlow, et. al., 2023).
Psychotherapy
Psychotherapy when supplemented with medication is the best combo for treating mood disorders. It is important to fix the chemical issue but one also needs to have a strong understanding of self and ways to think differently. Cognitive Behavioral Therapy plays a key role in helping individuals reframe and rethink distortions and negative connotations about self. An individual who is depressed already has negative connotations about self, the world and the future. AIHCP has blogs about CBT and its importance as a behaviorist therapy stemming from Aaron Beck and Albert Ellis that looks to help individuals think more healthy for better behavior and mental functioning. In addition, human centered therapies which gravitate towards self esteem and congruence and fulfillment are important. Karl Rogers and his person-centered therapy looks to support the client in meeting fulfillment through empathy, genuineness and unconditional positive regard. AIHCP also has a blog to review on human-centered therapies. Finally, interpersonal skills and support is key. Individuals suffering from loss need support. An individual with better support systems can overcome different losses with more success. Some have stronger internal systems of meaning and spirituality, while others may have more family or friends or financial means to overcome loss. Basic grief counseling in these ways can help individuals become more resilient when depressed or sad.
Conclusion
Please also review AIHCP’s Grief Counseling Program
Mood disorders can be stable with only one extreme or unstable and shift from mania to melancholy. They are among, with anxiety, the most common psychopathologies. Unfortunately, many individuals avoid treatment due to social stigma. It is important to find the time to take care of one’s mental health if afflicted with a mood disorder. Mood disorders can be genetic or causal but most all have solutions via medication, psychotherapy and counseling, or an integrated approach.
Please also review AIHCP’s Grief Counseling Certification as well as AIHCP’s multiple other behavioral health certification programs.
Clinical Depression (Major Depressive Disorder). (2026). Cleveland Clinic. Access here
Dimaria, L. (2026). “Types of Mood Disorders”. VeryWellMind. Access here
References
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorder” DSM-5-TR (5th ed., text revision). American Psychiatric Association Publishing.
Barlow, D.H., Durand, V.M., & Hofmann, S.G. (2023). Psychopathology. An integrative approach to mental disorder (9th ed.). Cengage Learning
McRay, B.W., Yarhouse, M.A., Butman, R.E., & Kiple, C. (2016). Modern psychopathologies: A comprehensive Christian appraisal. (2nd, ed.) IVP Academic
For some individuals depression does not seem to go away when treated initially. After multiple SSRI fail to work and if counseling fails to produce results, then other ways will be needed to help the person get through the depression. This video looks at resistant treatment depression and some ways individuals can find a way to overcome depression
Please also review AIHCP’s Grief Counseling Certification and see if it meets your academic and professional goals. The programs are online and independent study and open to qualified professionals seeking a four year certification
In the area of grief and loss, anxiety, trauma, or in special needs, individuals are or can become more closed off from other human beings. Many are unable to express emotions properly, communicate with others, or feel independent to do things or interact with others. Individuals can become closed off to the world and unable to communicate with it. Counselors can utilize a variety of the therapies to help individuals cope better with emotions and also open back up with the world, but sometimes, especially in the case of those with mental defect, individuals need other ways to communicate and express emotion.
Animals and pets can help individuals suffering from anxiety and depression find healing. Please also review AIHCP’s Grief Counseling Certification
Animals and pets are an excellent source of love and way to heal. Animals can bring out the best in people and their presence can reduce stress and depression. Animals hence can play a key role in helping individuals who are grieving or dealing with anxiety.
Animal Therapy for Grief, Depression and Anxiety
Animal Therapy is broad spectrum approach to healing and helping those with autism express themselves, but also those who have experienced trauma, or even those who have anxiety or depression issues. Animals help individuals in a broad variety of ways to rediscover self, heal and move forward. While those who face life long mental issues can gradually improve through animal therapy, those with trauma or temporary issues can also benefit greatly with the company of an animal.
Animal Therapy has a long history, back to even Sigmund Freud, and with the advances of the its modern father, Boris Levinson. The idea of the comforting nature of an animal or pet and his/her presence has a calming effect on human beings. The company of animals can increase serotonin and dopamine, as well as lower cortisol levels by awakening the para sympathetic system. The presence releases tension and allows the person to find healing.
There is no limit to the types of animals that can be utilized. Horses, dogs, cats, rabbits, ferrets and other small mammals, birds, fish and even lizards can all be utilized. Different species have different end goals that can help individuals with particular needs. Dogs play a key role providing comfort and unconditional love, while cats help with individuals who are more awkward with initial touch and need. Horses and equine therapy play a large role in animal therapy and are provided at various locations for those who need to form better connections, trust, and responsibility. Even birds or fish can play a role in helping individuals find connection but also responsibility.
Benefits of Animal Therapy
Animal Therapy helps those with a wide variety of mental issues, but also those dealing with stress, anxiety, loss and depression. Physically, animal therapy, reduces stress and lowers blood pressure and increases dopamine and serotonin. It reduces cortisol and helps the person find comfort and calm. Emotionally, animal therapy, helps individuals find love and support. The unconditional love an animal can supply, or the fact, the animal needs the person, can help the individual feel love when sometimes love is absent in the person’s world.
Psychologically, animals help individual feel love and from that love individuals can find stronger self esteem to feel loved but also to express love to a fellow creature. The need and dependency of the animal upon the person helps build the person’s purpose. In addition, this purpose gives the person duty and responsibility. During therapy, the person is called to care for the animal, supply food and water, or provide basic care such as grooming or walking. Even the smallest duty of having to feed a fish and supplying a need to another creature can have huge therapeutic effects on the person. This sense of purpose also increases self esteem especially with the depressed.
Animals can help the bereaved form new bonds, feel loved and find purpose again
In addition, training and teaching an animal helps individuals improve communication skills, social interaction, and independence to push forward in an endeavor or task. Individuals plagued with depression or other psychological maladies may be less receptive to enter the social arena of human interaction, but through animals, they can find it easier to communicate, wake up and do tasks, and exercise. This also increases one’s sense of trust between another being. Horse riding, or walking form bonds of trust which may be difficult with another person. This trust permits the person to feel more safe in social settings and to put oneself into the hands of another while also giving purpose to care for the other. Individuals experiencing loss may need to form new bonds and the bonds of love and trust and the social skills that are re-introduced through animals can be physically, emotionally and mentally rewarding.
Overall, animal therapy helps form new bonds, increases social interaction, improves communication skills, teaches trust and responsibility and reduces the physical manifestations of stress and anxiety. It gives the person purpose and responsibility again and helps the person re-enter the social world of other human beings or at least better skills to reintegrate oneself into society after trauma or loss, or if dealing with a mental issue. Animal Therapy can help with emotional release, talk therapy, and relief of various negative symptoms.
Obviously animal therapy is not for everyone. Some individuals may have issues that may endanger the animal, or others may be allergic to certain animals. Like all therapies, it depends upon the person but overall animal therapy is a very successful therapy when applied. One can find animal therapy through the referral of a therapist. Many are offered through campuses, hospitals and special programs at rehab centers or correctional facilities.
Conclusion
Animal Therapy can be supplemental with other therapies or a sole therapy. Ultimately, those with deeper issues such as Autism or permanent conditions can benefit greatly from animal therapy. Animals have the ability to help individuals form new bonds, express feelings and explore new skills necessary in social settings. Animals have the ability to bring out physical and emotional wellness by reducing stress and anxiety. Those who experience grief and loss can also form new bonds and find new purpose through animal care and the reciprocity of love that is shared between a person and animal. While animal therapy may not be the answer for everyone, it is highly successful for those suffering from various mental ailments and temporary issues with anxiety or depression.
Horses can play a large role in animal therapy. Please also review AIHCP’s Grief and Stress Management programs
Please also review AIHCP’s mental and behavioral health certifications, as well as in particular, it’s Grief Counseling Certification as well as its Stress Management Certification. The programs are online and independent study with mentorship as needed and is open to qualified professionals in the Healthcare, Human Service and Ministry fields. Please review and see if the programs meet your academic and professional goals.
Additional Resources
Baer, B. (2024). “Animal-assisted therapy (AAT) and emotional support animals”. Therapist.com. Access here
Jelinek, J. (2022). “All About Animal-Assisted Therapy”. PsychCentral. Access here
“Emotional Support/Therapy Animals”. (2017). Good Therapy. Access here
Olivine, A. (2024). “What Is Animal Therapy?” Very Well Health. Access here
“Animal-Assisted Therapy” (2022). Psychology Today Staff. Psychology Today. Access here
Carl Rogers, the famous psychologist and counselor, in the 1950s presented a far different approach than past Freudian psychological views that emphasized psycho-analysis and subconscious treatments. Like others, he wanted to approach counseling and the patient differently. He emphasized a more Humanistic approach that involved patient or client-centered therapies that addressed the feelings that existed now within the client. In an earlier blog, AIHCP discusses in a broader stroke the Humanistic approach to grief and counseling, but in this short blog, we will instead focus more solely on Rogerian concepts in helping individuals express feelings, in particular feelings associated with depression. Please also review AIHCP’s numerous counseling certifications for Human Service professionals.
Rogerian Theory
While Cognitive Behavioral Therapy looks to restructure and reframe illogical and negative emotional schemas with healthy and positive thoughts to alter behavior, Rogerian approaches look to address the the feelings of the client him/herself with unconditional love, genuineness, empathy and support. It looks to transform and strengthen the person. The term “client” is utilized instead of “patient” to remove stigmas that the person is sick or ill but merely needs love and guidance for life altering change. The counselor guides the client but the client ultimately has more control in the sessions and is able to express and discuss his/her feelings within a far less structured environment. Narrative is key. The counselor does not look to confront, but to listen.
Rogerian approaches in counseling are client centered and focuses in an empathetic and non-judgmental way the feelings of the client. Please also review AIHCP’s Grief Counseling Certification
Roger’s goal was to help the client reach self-actualization of what the person can become through a process of helping the client see him/herself as he/she is, wishes to be and how to become. Within this, a client learns to discover one’s self worth. The counselor also helps the client distinguish between self image and real image and how to reach the ideal image. When dealing with many individuals suffering with depression, self worth is something that is greatly damaged. Many depressed individuals feel they have very little worth or value. Whether this is due to something that occurred or merely depression without correlation to direct loss, the person feels a blanket of darkness over him/herself. Allowing the client to express these emotions, both positive and negative are key in Rogerian approaches. The counselor listens to these concerns with congruence and empathy, allowing the client to express and discuss the sadness and low self worth. The counselor helps the client direct the session into accurately describing how he/she feels and also views oneself. Many who are depressed also possess a very low self image. In many cases, this self image is not properly balanced with reality. Various distortions will emerge that are tied to the person’s feelings. It is not necessarily the role of the Rogerian approach to reframe these immediate concerns as in CBT, but to help the client understand the feelings and empathetically listen and restate these feelings to help the client re-discover where this false self image and true image lie. The counselor’s ultimate goal is help the client find a genuine understanding of his/her real self despite feelings. The counselor then looks to help the client find the ideal self. In this way, one’s self image and ideal self can become congruent and tied together.
Once congruence is established where the depressed individual is able to find self image and ideal image as a true reality, Rogers speaks of the possibility of self actualization where the person is able to thrive and exist again in an emotionally healthy way. Rogers listed five particular qualities of a fully functioning person who has tied self image and ideal together via self actualization. First, he pointed out that the person is open again to new experiences. Many depressed individuals are afraid to move on or seek out new things. A healthy functioning individual is able to seek out and find new meanings through new experiences. Second, Rogers spoke of existential living, where the person lives in the present and is able to experience the present in new fresh ways without prejudice or fear of the past. Many times, depressed individuals cannot untie themselves from the past and are unable to experience the present. Third, Rogers remarked that those who are functioning at a healthy level trust their feelings. Individuals are able to make decisions with certitude without doubt and not second guess oneself. Depressed individuals usually labor with decisions and fear what others may think or if they may fail. Fourth, Rogers pointed out that individuals should be creative without fear and able to move forward and share thoughts and ideas without fear of fallout from others. Depressed individuals lack the confidence to create or stand out. Finally, Rogers illustrated the idea of a fulfilled life where an individual is able to live life to its fullest. The person is able to find satisfaction in decisions, goals and challenges. Depressed individuals are unable to find joy in little things, much less have the energy for goals or the ability to face challenges.
These five qualities of a fully functional person are critical to overcoming the depressed state. When individuals are able to express these points within life, then they are again functional and free of the dark grip of depression. We will now in the next half of the blog look at how to implement Rogerian concepts and put them into practice. This will involve reviewing and understanding the basics of client-centered attending and responding skills.
Rogerian Practice
It is once congruence occurs and emotions are faced that the client is able to reach this type of fulfillment. The long process of helping the client discover this congruence and self-actualization is the key . While those who study the Rogerian approach understand the theory, it is the practical approach from person to person that is key.
Attending and Responding Skills are imperative in Rogerian Counseling. Please also review AIHCP’s Grief Counseling Certification
The counselor within the Rogerian approach utilizes a variety of micro counseling skills discussed in previous AIHCP blogs. Within Rogerian practice, basic attending skills are critical in helping the client discuss emotions and properly relate those emotions back. The counselor attends the client with empathetic listening. Rogers believed that genuine and empathetic listening was the first key in learning the story of the client. This involved active and intense focus on the client. The counselor should not only listen but show intense interest via eye contact, gestures, and physical positioning. In regards to response, the counselor looks not to judge the feelings of the client, but instead to restate or paraphrase them to the client. This helps the client not only understand that the counselor is listening but also to hear these feelings out loud. Sometimes, speaking about negative feelings also needs hearing them back to begin to decipher the false reality of those negative feelings. In essence, the empathetic approach of active listening and responding creates not only trust between client and counselor but also creates a safe zone where the client is able to fully express inner feelings. The counselor helps create this environment through multiple sessions and active and empathetic support for the client. The client feels he/she exists in a safe zone where no judgement or confrontation exists. It allows the client to take center stage and control and with the help of the counselor, unravel the negative emotions and find the real and possible ideal self that depression has hidden from the client. Rogers refers to this type of empathetic environment as one of unconditional love. It is place where feelings are not questioned or given positive or negative value, but only spoken about and understood within the context of the session. The counselor helps foster this environment because the counselor is not judging or giving qualitive value to the feelings. Instead the counselor is allowing the client to direct and discover value to the feelings.
Hence, how the counselor presents him/herself, listens, responds and creates a safe environment is critical to the success of Rogerian approaches. While the practice itself takes more time, seems unstructured, and is more about the now of emotion, it does have success with many patients facing depression and negative emotions. Obviously, sometimes supplemental approaches may be need introduced, as well as pharmaceutical remedies when issues beyond behavior exist such as neurological or hormonal, but overall, Rogerian approaches are very common place in counseling. The humanistic approach is very classical and non evasive for many individuals with already low self esteem issues that feel an abundance of negative emotions.
Those facing loss and depression need an empathetic ear and voice to help them heal. The emotional release and discussion of issues is a key part of grief healing. Through these discussions and release of emotions, the client can begin much of the grief work required that goes through the various emotional stages of denial, emotion, anger, and bargaining. The grief counselor utilizing Rogerian approaches will be able to listen as the person works through his/her grief and also notate any maladaptive emotions such as guilt that may appear. Through a non judgement zone, the counselor will be able to help the person come to grips with these emotions and help the person self-actualize beyond the loss or depression and find new hope.
Conclusion
Rogers client-centered care in the 1950s revolutionized counseling and forever changed how counselors approached clients. Humanistic approaches are in many ways the classical counseling sessions that individuals imagine where one speaks of feelings and the counselor paraphrases and asks how this makes one feel? It directly and openly deals with emotion without judgement and with complete empathy. This is a very important aspect to consider when dealing with depressed populations who may not be ready to deal with confrontations in counseling or face fast changes. Instead, the Rogerian approach gives the client control to discuss feelings and work them out. It slowly helps the client sort out negative feelings and replace them with positive vibes. The key is to help the client move forward in a productive and healthy life style that is congruent and true to self.
The counselor utilizes different micro counseling skills. The counselor refrains from direct reframing, or empathetic confrontations that may upset the client. Instead the counselor becomes more passive in direction and gently moves the client through good attending and responding skills that create a safe and no judgement zone. Depressed individuals, especially, need this type of environment to regain their voice and ability to move forward.
Please also review AIHCP’s numerous Human Service related certifications in counseling ranging from just not grief but also from stress to anger and crisis to spiritual counseling
Ultimately, as counseling continues, different techniques may need added to fit particular clients, or maybe even the necessity of medication, but overall, the initial Rogerian approaches will help the client feel safe and help form a strong bond between counselor and client.
If you would like to learn more about grief counseling, then please review the American Academy of Grief Counseling’s certification program in Grief Counseling. The program is online and independent study and open to qualified professionals seeking a four year certification as a grief counselor. AIHCP certified both pastoral counselors as well as clinical counselors. Bear in mind, certified grief counselors who are not licensed or clinical do face restrictions in what therapies they may utilize as well as treating complicated versions of grief that lead down trajectories that include depression.
AIHCP also offers a broad range of other Human Service counseling certifications that revolve around Anger Management, Crisis Intervention, Stress Management and both Spiritual Counseling and Christian Counseling.
References and Additional Resources
Mcleod, S. (2024). “Carl Rogers Humanistic Theory And Contribution To Psychology”. Simple Psychology. Access here
Bottaro, A. (2024). “Everything to Know About Person-Centered Therapy”. Very Well Health. Access here
Joseph, S. (2015). “Carl Rogers’ Person-Centered Approach”. Psychology Today. Access here
Hopper, E. (2018). “An Introduction to Rogerian Therapy”. Thoughtco. Access here
Miller, K. (2019). “Carl Rogers’s Actualizing Tendency: Your Ultimate Guide”. Positive Psychology. Access here
Treatment Resistant Depression can make one lose hope. Please also review AIHCP’s Grief Counseling Certification
Depression, a debilitating mental health condition, significantly impacts the lives of millions worldwide. Among its most challenging forms is resistant treatment depression, where patients do not respond to traditional therapies. This complexity underscores the critical need for a deeper understanding of treatment resistant depression treatment options, guiding patients towards improved mental health outcomes. As the prevalence of this condition poses significant challenges to both patients and healthcare providers, exploring innovative methods and therapies becomes imperative.
The subsequent discussion in this article aims to shed light on various facets of resistant treatment depression, starting with a thorough understanding of what characterizes treatment-resistant depression and how it can be identified. It will delve into the risk factors associated with the development of this form of depression and examine both medication options and non-medication therapies and interventions. Furthermore, the role of psychotherapy in managing resistant treatment depression will be highlighted, alongside innovative and experimental treatments that hold promise for those affected. Lastly, the creation of personalized treatment plans will be discussed, emphasizing the tailored approach required to address the unique needs of each individual facing resistant treatment depression. This comprehensive exploration aims to equip readers with the knowledge to navigate the complexities of treatment-resistant depression treatment, advocating for a proactive and informed approach to mental health care.
Key Takeaways
Treatment-resistant depression (TRD) occurs when at least two different antidepressants fail to improve symptoms.
TRD affects about 30% of individuals with major depressive disorder.
There are multiple treatment strategies for TRD, including optimization, switching, combination, augmentation, and somatic therapies.
Non-pharmacological treatments such as psychotherapy, electroconvulsive therapy (ECT), and transcranial magnetic stimulation (TMS) can be effective.
Early diagnosis and personalized treatment plans are crucial for managing TRD effectively.
Also, please feel free to review AIHCP’s Grief Counseling Certification and see if it meets your academic and professional goals.
Understanding Treatment-Resistant Depression
Definition and Overview
Treatment-resistant depression (TRD) is a subtype of major depressive disorder (MDD) characterized by inadequate response to standard antidepressant therapies. Patients with TRD have undergone at least two different first-line antidepressant treatments without sufficient relief during a depressive episode. This condition is not only prevalent but also poses significant challenges in mental health care, affecting approximately 30% of individuals diagnosed with MDD. TRD often requires a comprehensive evaluation to understand the underlying factors contributing to its persistence. This may include reviewing the patient’s medical history, current medications, and adherence to prescribed treatments. Specialists might also explore other mental health conditions that could influence the depression’s responsiveness to treatment, such as bipolar disorder or personality disorders.
There are several misconceptions about TRD, including the belief that it is synonymous with “no hope.” In reality, there are multiple treatment options available, including medications and procedures like electroconvulsive therapy (ECT). Understanding these options can help dispel myths and encourage patients to seek comprehensive care.
The complexity of treatment-resistant depression requires a nuanced understanding and a personalized approach to treatment.
Prevalence and Impact on Individuals
The prevalence of treatment-resistant depression is alarmingly high, with estimates suggesting that at least 30% of persons with depression are affected by this condition. In some populations, such as those covered by Medicaid, the prevalence can be as high as 44.2%. The impact of TRD extends beyond the individual, affecting societal costs and healthcare utilization significantly. Individuals with TRD often experience more severe symptoms, longer depressive episodes, and a greater number of lifetime depressive episodes compared to those with non-resistant MDD. Additionally, TRD is associated with higher indirect costs due to increased disability benefits, workplace absenteeism, and the burden on caregivers. The healthcare costs and unemployment costs attributable to TRD are disproportionately high, reflecting the intensive treatment and support required for managing this condition. Furthermore, the rate of suicidality, including completed suicides, is markedly higher among populations with TRD, underscoring the urgent need for effective interventions and support systems.
Identifying Signs of Treatment-Resistant Depression
The biggest sign of treatment resistant depression is not feeling better
Lack of Improvement despite Treatment
Individuals experiencing treatment-resistant depression often find that standard treatments such as antidepressants or psychotherapy do not alleviate their symptoms effectively. Despite undergoing multiple treatments, their symptoms might not improve, or they may experience only temporary relief before their symptoms return. This persistent lack of response to conventional treatments is a hallmark of treatment-resistant depression, necessitating the exploration of alternative therapeutic approaches.
Persistent Symptoms and their Severity
Treatment-resistant depression is characterized by more severe symptoms compared to typical major depressive disorder. Individuals may suffer from prolonged depressive episodes and exhibit symptoms such as anhedonia, which is a reduced ability to experience pleasure. The severity of these symptoms often leads to significant impairment in daily functioning and quality of life. Additionally, individuals with treatment-resistant depression are more likely to experience increased anxiety and have a higher risk of suicidal ideation and behavior. These persistent and severe symptoms underscore the critical need for effective management strategies tailored to this challenging condition.
Clinical Evaluation
Treatment-resistant depression can be hard to diagnose. Sometimes, other conditions or problems can cause similar symptoms. So when you meet with your doctor, they will want to:
Review your experience with psychotherapy (talk therapy) and if it has helped manage depression.
Assess physical health conditions that can sometimes cause or worsen depression, like thyroid disease and chronic pain.
Assess issues like substance use problems.
Consider if a different mental health condition more accurately describes your symptoms, like bipolar disorder or a personality disorder.
Diagnostic Tools
Depression is a clinical diagnosis, based on the history and physical findings. No diagnostic laboratory tests are available to diagnose major depressive disorder. However, healthcare providers may use various screening tools and questionnaires to aid in the assessment.
Challenges in Diagnosis
The diagnosis of treatment-resistant depression isn’t clearly defined. But most healthcare providers diagnose TRD if your depression symptoms haven’t improved after trying at least two first-line antidepressant medications. Most providers consider the following to be first-line depression medications:
SSRIs
SNRIs
Bupropion
Mirtazapine
Accurate diagnosis is crucial for effective treatment planning and management of treatment-resistant depression.
Risk Factors for Developing Treatment-Resistant Depression
Genetic Predispositions
Genetic factors play a significant role in the development of treatment-resistant depression (TRD). Research indicates that first-degree relatives of individuals with TRD are at an increased risk for developing the condition themselves. This familial tendency suggests that genetic predispositions are influential in the resistance to antidepressant treatments. Furthermore, specific genetic polymorphisms, such as those found in the serotonin transporter (5-HTT) and the brain-derived neurotrophic factor (BDNF), have been linked to variations in treatment response. Polymorphisms in the 5-HTT promoter region and BDNF gene affect neurogenesis and the serotonergic system, which are crucial in the pathophysiology of depression and its treatment. Genetic predisposition plays a significant role in the development of treatment-resistant depression (TRD). Studies have shown that individuals with a family history of depression are at a higher risk of developing TRD. Specific genetic markers and variations can influence how patients respond to antidepressant medications, making it crucial to consider genetic factors in treatment planning.
Environmental and Lifestyle Factors
Environmental and lifestyle factors also contribute significantly to the risk of developing TRD. Patients with TRD often report a higher number of stressful life events, such as severe health conditions, financial stress, or significant interpersonal relationship problems. Additionally, lifestyle choices, such as moderate to heavy alcohol consumption, have been associated with poorer responses to treatment. Adverse childhood experiences, including trauma and bullying, have also been reported frequently among those with TRD, indicating that early life stressors can increase vulnerability to later life stressors and potentially lead to treatment resistance.
Patients with depression who have some medical illnesses—such as thyroid disease and chronic pain—are at greater risk for TRD. Other conditions associated with TRD include substance abuse and eating and sleep disorders, which have the potential to make you more prone to being resistant to treatment with antidepressants.
A depressed person’s overall health can also play a role. Addressing these comorbid conditions is essential for improving treatment outcomes in TRD.
By understanding the complex interplay between genetic predispositions and environmental factors, healthcare providers can better identify individuals at risk for TRD and tailor interventions that address these specific risk factors.
Exploring Medication Options
Switching Antidepressants
When patients exhibit poor response or intolerable side effects to an initial antidepressant, switching to another may be necessary. It is crucial for clinicians to be well-versed in the pharmacodynamics of each drug, aware of potential drug-drug interactions, and the expected timeline for the onset of the new medication’s effectiveness. Studies have shown that approximately 9% of patients undergoing antidepressant monotherapy switch to another antidepressant during treatment.
Pharmacological treatment strategies for treatment-resistant depression (TRD) involve a multi-faceted approach to manage symptoms effectively. Different antidepressants work in different ways to affect specific chemicals (neurotransmitters) that send information along brain circuits that regulate mood. If a current medication isn’t helping enough, other drugs might be considered.
First-Line Medications
First-line medications typically include selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs). These medications are often the initial choice due to their efficacy and safety profile. However, if these medications do not yield the desired results, other classes of antidepressants may be explored.
Combination Therapy
Combining antidepressants can offer a synergistic effect, enhancing efficacy or tolerability. For example, combining SSRIs, which extensively inhibit serotonin reuptake, with agents like trazodone or nefazodone that block 5-HT2A receptors can reduce agitation and insomnia, allowing for higher dosages and increased efficacy. Moreover, combinations like SSRIs with bupropion, which also targets noradrenaline and dopamine reuptake, have shown greater improvement in treatment-resistant depression. The use of lithium as an adjunct to antidepressants like TCAs, MAOIs, and SSRIs has been shown to enhance response rates and prevent early relapse by affecting various neurotransmitter systems and neuroplastic changes.
Novel Medications and Approaches
Esketamine, a component of ketamine, represents a novel approach in treating resistant depression. Approved as a nasal spray, it must be administered under clinical supervision due to potential side effects such as dissociation and extreme relaxation. Esketamine acts on the glutamate neurotransmitter system, differing from traditional antidepressants that primarily affect serotonin. This allows for the formation of new neural pathways, potentially preventing the recurrence of depression. Patients may notice rapid improvements, often within days, especially when esketamine is used in conjunction with traditional antidepressants.
Innovative combination therapies have also shown promise. For instance, the combination of the SSRI fluoxetine with olanzapine has been superior in treating resistant depression compared to either treatment alone. Similarly, augmentation strategies like adding triiodothyronine (T3) to TCAs have accelerated response times and have been particularly effective in women. The β-adrenergic/5-HT1A receptor antagonist pindolol has been used to enhance the effects of SSRIs by binding to 5-HT1A receptors, although results have been mixed.
Through a deeper understanding of these medication options and their mechanisms, clinicians can better tailor treatments to meet the unique needs of individuals with treatment-resistant depression.
Non-Medication Therapies and Interventions
Grief therapists can help individuals with a variety of therapies to help the person through the depression when medications fail to work
Psychotherapy Techniques
Psychotherapy remains a cornerstone in the management of treatment-resistant depression, offering various techniques tailored to individual needs. Cognitive-behavioral therapy (CBT) and interpersonal psychotherapy (IPT) have shown efficacy in treating mild to severe nonpsychotic major depression and, based on limited research, offer comparable benefits to medications in treatment-resistant cases. The integration of psychotherapy with usual treatment has been found to moderately improve outcomes compared to usual treatment alone, with effect sizes similar to those seen in adjunctive pharmacotherapies. Psychotherapies provide unique advantages, particularly for patients whose depressive episodes are linked to specific outlooks, symptoms, or stressors. Unlike medications, psychotherapies help patients structure their lives, enhance self-understanding, and improve interpersonal functioning.
Electroconvulsive Therapy (ECT) and Other Neuromodulation Therapies
Electroconvulsive therapy (ECT) is highly effective for severe depression and has a significant advantage over antidepressant medications in treatment-resistant cases. ECT involves administering electrical currents to induce a controlled seizure, significantly reducing depressive symptoms and enhancing response rates. The procedure’s safety has improved with the use of general anesthesia, muscle relaxants, and modern monitoring techniques. Other neuromodulation therapies such as repetitive transcranial magnetic stimulation (TMS) and deep brain stimulation (DBS) also offer promising results. TMS has consistently outperformed sham treatments in major depressive disorder, providing a non-invasive option with minimal side effects like transient headaches. DBS, though more invasive, targets specific brain areas with electrical impulses to alter neural activity and alleviate depression.
Lifestyle Changes and Complementary Therapies
Addressing lifestyle factors plays a critical role in managing treatment-resistant depression. Regular physical activity, adherence to a Mediterranean diet, maintaining good sleep hygiene, and ensuring sufficient sunlight exposure are recommended as part of a comprehensive treatment plan. These interventions not only support overall health but also directly impact depression symptoms by reducing stress, improving sleep, and enhancing mood. Complementary approaches such as acupuncture, although less effective in treating depression directly, may offer additional health benefits. The use of supplements like omega-3 fatty acids, and St. John’s wort has shown mixed results, necessitating careful consideration of potential interactions and benefits. Moreover, light therapy can be particularly beneficial for those experiencing seasonal exacerbations of depression.
The Role of Psychotherapy in Managing Treatment-Resistant Depression
Cognitive Behavioral Therapy (CBT)
Cognitive Behavioral Therapy (CBT) is a prevalent form of psychotherapy that addresses the interconnections between thoughts, feelings, and behaviors that affect mood. It is specifically designed to identify and modify distorted or negative thinking patterns and teaches individuals skills to respond positively to life’s challenges. This therapy is particularly effective for those suffering from treatment-resistant depression, as it provides them with tools to manage their depressive symptoms actively. The therapy focuses on altering negative thought patterns, improving interpersonal relationships, and developing coping strategies.
Other Therapeutic Approaches
Several other psychotherapeutic approaches play crucial roles in managing treatment-resistant depression. Acceptance and Commitment Therapy (ACT), a branch of CBT, encourages patients to accept their thoughts and feelings rather than fighting them, promoting positive behavioral changes even in the presence of negative thoughts. Interpersonal Psychotherapy (IPT) focuses on resolving interpersonal issues contributing to depression, helping patients improve their relationship dynamics.
Family or marital therapy involves the patient’s family members or partners in the therapeutic process. This approach is beneficial as it addresses and works through relationship stress that may be impacting the patient’s depression. Dialectical Behavioral Therapy (DBT) is another effective method, particularly for those with chronic suicidal thoughts or behaviors associated with treatment-resistant depression, as it combines acceptance strategies with problem-solving skills.
Group psychotherapy offers a unique environment where individuals with depression can interact with others facing similar challenges, facilitated by a psychotherapist. This setting can enhance support and sharing of coping strategies among participants.
Mindfulness and Behavioral Activation are also valuable in the treatment arsenal against resistant depression. Mindfulness encourages individuals to be present and non-judgmental about their thoughts and feelings, which can help manage stress and depressive symptoms. Behavioral Activation helps patients engage in activities that improve mood and reduce isolation, gradually reversing the withdrawal that often accompanies depression.
Each of these therapies provides distinct benefits and can be tailored to meet the specific needs of individuals dealing with treatment-resistant depression, underscoring the importance of a personalized approach in psychotherapeutic interventions.
Innovative and Experimental Treatments
Ketamine and Esketamine
Esketamine, approved by the US Food and Drug Administration (FDA) and European Medicines Agency (EMA) in 2019, is a novel pharmacological agent recognized for its glutamatergic neuromodulatory properties. It functions through non-selective, non-competitive antagonism of N-methyl-D-aspartate (NMDA) receptors, which are crucial for mood regulation and emotional behavior. This antagonism results in a transient increase in glutamate release, stimulating further neurotransmitter activity that is vital for combating depressive symptoms. Esketamine’s rapid onset is linked to its ability to stimulate the mammalian target of rapamycin complex 1 (mTORC1), promoting synaptogenesis and enhancing brain-derived neurotrophic factor production, which are essential for effective treatment outcomes in treatment-resistant depression (TRD).
The intranasal form of esketamine is particularly noted for its quick action, often showing antidepressant effects shortly after administration, which is critical for patients with severe depression or those at imminent risk of suicide. However, its use must be carefully monitored due to potential psychotomimetic effects, and it is generally administered in a clinical setting to manage these risks effectively.
Psychedelic-Assisted Therapy
In recent years, there has been a significant resurgence of interest in the use of psychedelic compounds, such as psilocybin, for treating mental disorders like TRD. Psilocybin, found in magic mushrooms, has been studied in various clinical settings, often in conjunction with supportive psychotherapy. It has demonstrated substantial antidepressant effects in both open-label and randomized controlled trials, although these studies often face limitations such as small sample sizes and lack of rigorous control conditions.
Psilocybin’s effects are believed to stem from its activation of serotonin 2A (5-HT2A) receptors, leading to altered states of consciousness, or the ‘psychedelic trip,’ which is central to its therapeutic potential. Current research is exploring whether these effects can be separated from the psychedelic experience, with studies like the proof-of-concept randomized controlled trial combining psilocybin with risperidone to block the psychedelic effects and assess the antidepressant potential in isolation.
Moreover, patient feedback suggests the need for more personalized approaches in psychedelic-assisted therapy, emphasizing trust-building, individualized preparation, and the possibility of multiple treatment sessions to optimize the therapeutic outcomes for TRD. This patient-centered feedback is crucial for refining treatment protocols and enhancing the adaptability of psychedelic therapies in clinical practice.
The future of treating depression lies in the continuous exploration of new therapies and the rigorous testing of their effectiveness and safety.
Creating a Personalized Treatment Plan
Working with a Specialist
When experiencing persistent symptoms of depression despite ongoing treatment, it is crucial to consult a specialist who can provide a comprehensive review and adjustment of the current treatment plan. Specialists, such as psychiatrists or psychiatric nurse practitioners, are equipped to assess the effectiveness of current treatments and make necessary changes. They may review the patient’s medical history, inquire about life situations impacting the depression, and consider any physical health conditions that could influence symptoms. Additionally, they might adjust medications, suggest different therapeutic approaches, or recommend advanced treatments like repetitive transcranial magnetic stimulation (rTMS) or electroconvulsive therapy (ECT) if standard therapies are ineffective.
Evaluating and Adjusting the Treatment Plan
Creating an effective treatment plan for depression involves continuous evaluation and flexibility to adapt to the patient’s evolving needs. This may include altering the treatment setting, the types of medications used, and the psychological treatments applied. Patients and caregivers should be actively involved in this process to ensure that the plan remains practical and applicable to the patient’s specific circumstances. Regular follow-ups with the healthcare provider are essential to assess the treatment’s effectiveness and to make timely adjustments. This collaborative approach helps in maintaining a strong therapeutic alliance, which is vital for encouraging patient adherence and ultimately improving treatment outcomes.
Support Systems and Self-Care Strategies
Incorporating support systems and self-care strategies into the treatment plan is fundamental for individuals with treatment-resistant depression. Engaging in regular physical activity, maintaining a balanced diet, and ensuring adequate sleep are critical components that enhance the overall effectiveness of medical treatments. Patients are encouraged to manage stress through mindfulness and relaxation techniques, which can significantly alleviate symptoms of depression. Support from family, friends, and community resources also plays a crucial role in recovery. Educational programs about depression can help patients and caregivers recognize early signs of relapse and seek prompt treatment, reducing the risk of complications.
By integrating these approaches, a personalized treatment plan for depression not only addresses the medical and psychological aspects of the condition but also empowers individuals to take proactive steps towards their mental health and well-being.
Management and Long-Term Care
Long term care is sometimes required to help someone with treatment resistant depression
Personalized Treatment Plans
Management of treatment-resistant depression (TRD) requires personalized treatment plans tailored to the individual needs of each patient. These plans often involve a combination of pharmacological and non-pharmacological strategies to address the complex nature of TRD. Regular assessment and adjustment of the treatment plan are crucial to ensure its effectiveness and to minimize side effects.
Monitoring and Follow-Up
Continuous monitoring and follow-up are essential components of managing TRD. This includes regular appointments with healthcare providers to evaluate the patient’s progress and to make necessary adjustments to the treatment plan. Monitoring should also involve tracking any side effects and the overall impact of the treatment on the patient’s quality of life.
Patient and Family Support
Support from family and caregivers plays a significant role in the long-term management of TRD. Providing education about the condition and involving family members in the treatment process can enhance the effectiveness of the treatment plan. Additionally, support groups and resources can offer emotional and practical assistance to both patients and their families.
Effective management of treatment-resistant depression requires a comprehensive approach that includes personalized treatment plans, continuous monitoring, and robust support systems.
Living with Treatment-Resistant Depression
Living with treatment-resistant depression (TRD) presents unique challenges that require a multifaceted approach to manage effectively. Arriving at the right treatment can take some trial and error. However, persistence and a comprehensive, patient-centered approach can lead to significant improvements in quality of life.
Ethical and Societal Considerations
Access to care for individuals with treatment-resistant depression is a significant ethical concern. Disparities in healthcare access can exacerbate the condition, particularly in low- and middle-income countries. Ensuring equitable access to innovative treatments is crucial for global health equity.
Stigma surrounding mental health remains a pervasive issue. It can deter individuals from seeking help and contribute to the worsening of symptoms. Combatting stigma requires a multifaceted approach, including public education and policy changes.
Effective policy and advocacy are essential for addressing the needs of those with treatment-resistant depression. This includes advocating for responsible supply bases and supplier-enabled innovation to ensure that new treatments are both ethical and accessible. Policymakers must consider the psychiatric and legal considerations for novel treatments to ensure they are implemented responsibly.
Addressing ethical and societal considerations is not just a medical challenge but a moral imperative. It requires collaboration across sectors to create a supportive environment for those affected by treatment-resistant depression.
Prevention and Early Intervention
Identifying early warning signs of treatment-resistant depression is crucial for timely intervention. Early detection can significantly improve treatment outcomes and reduce the disease recurrence rate. Common early warning signs include persistent sadness, loss of interest in activities, and changes in sleep patterns.
Preventive strategies play a vital role in managing treatment-resistant depression. These strategies include:
Regular mental health screenings
Stress management techniques
Healthy lifestyle choices, such as regular exercise and a balanced diet
Building strong social support networks
Primary care providers are often the first point of contact for individuals experiencing depressive symptoms. They play a critical role in early intervention by:
Conducting thorough clinical evaluations
Utilizing diagnostic tools to assess the severity of depression
Referring patients to mental health specialists when necessary
Effective collaboration between primary care providers and mental health specialists is essential for comprehensive care.
By implementing these preventive strategies and recognizing early warning signs, healthcare professionals can better manage and treat treatment-resistant depre
Conclusion
Please also review AIHCP’s Grief Counseling Certification and see if it meets your academic and professional goals
Throughout this exploration of resistant treatment depression, we’ve traversed a vast landscape of innovative methods and therapies that spotlight the pressing need for personalized and comprehensive approaches. From the nuances of identifying treatment-resistant depression, understanding its risk factors, to the meticulously discussed medication options and non-medication therapies, the article offers a beacon of hope for those navigating this challenging condition. It underscores the crucial role of psychotherapy, alongside the promising horizon of experimental treatments like esketamine and psychedelics, in crafting a tailored treatment plan that resonates with the unique experiences and needs of each individual.
The journey towards conquering treatment-resistant depression is a testament to the resilience of both patients and healthcare providers in the face of adversity. It is a reminder of the importance of continuing research, patient-centered care, and the amalgamation of traditional and novel therapies to enhance mental health outcomes. By fostering a deeper comprehension of this condition and advocating for a multifaceted approach to treatment, we pave the way for more effective management strategies and a future where the shadows of resistant treatment depression are illuminated by the light of hope and healing.
Please also review AIHCP’s Grief Counseling Certification. Licensed counselors as well as pastoral counselors can both earn a Grief Counseling Certification to aid in their pastoral ministry or in licensed field of counseling. Remember, grief counseling outside the licensing arena cannot go beyond pathology. Hence pastoral counselors cannot help clients with depression and need to refer them to clinical and licensed counselors. AIHCP’s program covers numerous aspects of grief as well as depression but the certification itself is not a licensure and does not provide the rights that correspond with a licensed counselor. So when dealing with depression issues, pastoral counselors need to be careful not to treat but to refer.
AIHCP’s program in Grief Counseling is online and independent study and leads to a four year certification.
Frequently Asked Questions
What is treatment-resistant depression?
Treatment-resistant depression (TRD) is a type of major depressive disorder that does not respond to at least two different antidepressant treatments of adequate dosage and duration. The most effective management strategy for treatment-resistant depression often involves a combination of psychotherapy and medication. This approach not only addresses the chemical imbalances in the brain but also helps uncover and tackle underlying issues contributing to the depression. Through therapy, individuals can learn practical behaviors and strategies to combat their depression.
How common is treatment-resistant depression?
Treatment-resistant depression affects about 30% of people diagnosed with major depressive disorder.
What are the primary symptoms of treatment-resistant depression?
The primary symptoms include persistent feelings of sadness, loss of interest in activities, and difficulty concentrating, despite treatment efforts.
What are the treatment options for treatment-resistant depression?
Treatment options include optimizing current medications, switching medications, combination therapies, augmentation strategies, and non-pharmacological treatments like psychotherapy and electroconvulsive therapy (ECT). The latest advancement in treating treatment-resistant depression is Transcranial Magnetic Stimulation (TMS). This innovative, non-invasive method involves using gentle pulses of magnetic fields to stimulate nerve cells in the brain. It offers a different mechanism of action compared to traditional antidepressants like serotonin reuptake inhibitors (SSRIs) and does not come with their common side effects, including weight changes and sexual dysfunction.
What are the risk factors for developing treatment-resistant depression?
Risk factors include genetic predisposition, environmental influences, and comorbid conditions such as anxiety or substance abuse.
How is treatment-resistant depression diagnosed?
Diagnosis typically occurs after a patient has not responded to two different first-line antidepressant medications taken for a sufficient duration, usually six to eight weeks.
Are there non-medication options for treating treatment-resistant depression?
Yes, non-medication options include psychotherapy approaches, electroconvulsive therapy (ECT), and transcranial magnetic stimulation (TMS).
What should I do if I suspect I have treatment-resistant depression?
Consult with a healthcare provider who can perform a thorough evaluation and work with you to develop a personalized treatment plan. There is new hope for individuals struggling with treatment-resistant depression. The Treatment-Resistant Depression (TRD) Neuromodulation Clinic is at the forefront of offering innovative treatments such as repetitive Transcranial Magnetic Stimulation (rTMS) and esketamine. These treatments are specifically designed for veterans and others whose depression has not improved after several attempts with traditional antidepressant medications.
Additional Resources
“Treatment-Resistant Depression: What We Know and How To Manage It”. (2022). Cleveland Health Essentials. Cleveland Clinic. Access here
Bruce, D. (2023). “Treatment-Resistant Depression” WEBMD. Access here
Meissner, M. (2021). “What To Do When Your Antidepressant Isn’t Helping Enough”. PsychCentral. Access here
“How to Manage Treatment-Resistant Depression” (2023). Healthline Medical Network. Healthline. Access here
SAD or Seasonal Affective Disorder is a type of depression that coincides with the change of seasons. It can be during any type of season but primarily occurs during the Winter months. It is quite different than the Winter Blues in that it is consistent every year. It is hard enough without longer days and sunlight to function but with Winter, especially after the Holidays, many will fall into SAD.
Individuals can find help, medication, as well as light therapy to help. It is important to identify if you do have SAD and find the appropriate help from a licensed counselor who can guide you in the right direction. SAD is more than being upset about the weather but a type of depression that needs professional care. Please also review AIHCP’s Grief Counseling Certification. While certified grief counselors who are not licensed counselors as well cannot treat depression, they do have the training to spot it and send you to a professional counselor who can treat it.
AIHCP’s Grief Counseling Certification is online and independent study and open to qualified professionals. Please review the program and see if it meets your academic and professional goals.
While having a child is supposed to be the most exciting and wonderful thing in life, sometimes after the birth of a child, the mother, or even the father, can experience sadness and even depression. This is not due to actual loss but a chemical imbalance within the neurotransmitters that is offset. In mothers, it can be due to a variety of hormonal issues, while in fathers, it can be due to past depression history. “Baby Blues”, when it does occurs, lasts anywhere from a few days to a two weeks, but if it persists into depression, it is important to seek help from one’s doctor to help properly balance oneself. This is why it is so important for spouses, family and friends to observe each other during the first few weeks after child birth. Usually the emphasis is on the infant only but changes in mood for parents are also important things to watch and monitor. This type of situation is not anything to be ashamed of or a dismissal of the joyous occasion, but merely is mental health and properly taking care of it.
Postpartum Depression can rob one of the joy of having a child. It is important to seek medical help if symptoms persist for more than 2 weeks
Many of the symptoms associated with Post Partum Depression mirror any other type of depression but the biggest issue is it prevents proper bonding with one’s child and can make it harder to meet the needs of the new infant. This happy moment should be an experience of joy, but when depression sinks in, it can be difficult to enjoy these memorial moments or even worst, cause risk to self or the child. This is why it is so critical to seek help.
The article, “Post Partum Depression” from the Mayo Clinic takes a closer look at issues surrounding sadness, depression or even psychosis after child birth. The article states,
“The birth of a baby can start a variety of powerful emotions, from excitement and joy to fear and anxiety. But it can also result in something you might not expect — depression. Most new moms experience postpartum “baby blues” after childbirth, which commonly include mood swings, crying spells, anxiety and difficulty sleeping. Baby blues usually begin within the first 2 to 3 days after delivery and may last for up to two weeks. But some new moms experience a more severe, long-lasting form of depression known as postpartum depression”.
“Post Partem Depression”. Mayo Clinic. (2022). Mayo Clinic
Becoming a mother is a life-changing experience, but it can also bring about unexpected challenges. One such challenge is postpartum depression, a condition that affects many women after giving birth. Understanding postpartum depression is the first step towards finding effective strategies to deal with it. Postpartum depression is not simply a case of “baby blues” or feeling a bit down; it is a serious mental health condition that requires attention and support.
Postpartum depression can manifest in different ways, but some common signs and symptoms include persistent feelings of sadness, anxiety, and irritability. Women experiencing postpartum depression may also struggle with sleep disturbances, changes in appetite, and a lack of interest in activities they once enjoyed. It’s important to recognize these symptoms and seek help if they persist for more than a couple of weeks. Postpartum depression can have a profound impact on a mother’s overall well-being, as well as on her relationships and family dynamics.
The impact of postpartum depression on mothers and families
Postpartum depression not only affects the mother, but it can also have a significant impact on her relationships and family. The emotional and physical toll of postpartum depression can strain the bond between the mother and her partner, leading to feelings of isolation and resentment. In some cases, postpartum depression can even affect the mother’s ability to bond with her newborn baby, potentially impacting the child’s development.
Post Partum Depression can cause major strains on families after child birth and also play a role in not providing the infant with the care he/she needs
Furthermore, postpartum depression can disrupt the entire household dynamic. Partners may need to take on additional responsibilities, and other family members may need to step in to provide support. This can create stress and tension within the family, further exacerbating the challenges faced by the mother. Recognizing the impact of postpartum depression on mothers and families is crucial in order to provide the necessary support and understanding during this difficult time.
Effective strategies for dealing with postpartum depression
Dealing with postpartum depression requires a multi-faceted approach that addresses both the physical and emotional aspects of the condition. While it is important to seek professional help, there are also effective strategies that can be implemented on a daily basis to manage symptoms and promote recovery.
One such strategy is self-care. Taking care of oneself is often overlooked when dealing with postpartum depression, but it is essential for the mother’s well-being. This can include engaging in activities that bring joy and relaxation, prioritizing sleep and nutrition, and finding ways to manage stress. Self-care is not selfish; it is a necessary step towards healing and recovery.
Building a support system is another crucial aspect of dealing with postpartum depression. Surrounding oneself with understanding and supportive individuals can make a world of difference. This can include reaching out to family and friends, joining support groups specifically for postpartum depression, or connecting with other mothers who have gone through similar experiences. Having a support system in place provides a sense of validation and helps combat feelings of isolation.
Seeking professional help for postpartum depression
While self-care and support systems are important, it is essential to seek professional help when dealing with postpartum depression. Mental health professionals, such as therapists or counselors specializing in postpartum depression, can provide the necessary guidance and support. They can help identify underlying causes, develop coping mechanisms, and provide effective treatment options.
Antidepressant medication may also be prescribed in some cases, especially if the symptoms of postpartum depression are severe. It is important to consult with a healthcare provider to determine the best course of action. Seeking professional help is not a sign of weakness; it is a proactive step towards recovery and empowerment.
Support groups and resources for postpartum depression
Support groups can be a valuable resource for women dealing with postpartum depression. These groups provide a safe and understanding space where mothers can share their experiences, receive support, and learn from others who have faced similar challenges. Support groups can be found both online and in-person, offering flexibility and accessibility.
There are also numerous resources available for women experiencing postpartum depression. Websites, books, and podcasts dedicated to postpartum depression provide valuable information and strategies for coping. Additionally, many organizations offer helplines and online chat services where women can seek guidance and support in real-time. Utilizing these resources can help women feel empowered and less alone in their journey towards recovery.
Self-care tips for managing postpartum depression
Self-care is an essential component of managing postpartum depression. Here are some practical self-care tips that can be incorporated into daily routines:
Prioritize sleep: Aim for quality sleep by establishing a regular sleep schedule and creating a relaxing bedtime routine.
Nourish your body: Focus on eating a balanced diet that includes nutrient-rich foods to support overall well-being.
Engage in gentle exercise: Physical activity, such as yoga or walking, can help boost mood and reduce stress.
Practice mindfulness: Incorporate mindfulness techniques, such as deep breathing or meditation, to promote relaxation and reduce anxiety.
Delegate and ask for help: Don’t be afraid to ask for assistance from loved ones or hire help with household tasks to alleviate some of the pressure.
Engage in activities you enjoy: Make time for hobbies or activities that bring you joy, whether it’s reading, painting, or listening to music.
Remember, self-care is not a luxury but a necessity for your well-being. By prioritizing self-care, you are better equipped to navigate the challenges of postpartum depression.
Building a support system for postpartum depression
Building a support system is crucial for women dealing with postpartum depression. Here are some strategies for creating a strong support network:
Communicate with your partner: Openly discuss your feelings with your partner and seek their understanding and support.
Reach out to family and friends: Share your experiences with trusted loved ones who can provide emotional support and practical assistance.
Join support groups: Connect with other women experiencing postpartum depression through local support groups or online communities.
Seek professional help: Consult with mental health professionals who specialize in postpartum depression for guidance and support.
Consider therapy for couples: Couples therapy can help improve communication and strengthen the relationship during this challenging time.
Remember, you don’t have to face postpartum depression alone. Building a support system can provide the encouragement and understanding you need to navigate this difficult period.
Creating a postpartum depression action plan
Creating an action plan can help you navigate the challenges of postpartum depression proactively. Here are some steps to consider when developing your plan:
Educate yourself: Learn about postpartum depression, its symptoms, and available resources.
Set realistic goals: Break down your recovery journey into manageable steps to avoid feeling overwhelmed.
Identify triggers: Recognize the situations or circumstances that worsen your symptoms, and develop strategies to manage them.
Establish a routine: Creating a daily routine can provide structure and stability during this unpredictable time.
Practice self-care: Incorporate self-care activities into your daily routine to prioritize your well-being.
Seek professional help: Consult with mental health professionals to develop a personalized treatment plan.
By creating an action plan, you are taking an active role in managing your postpartum depression and empowering yourself towards recovery.
Conclusion
Please also review AIHCP’s Grief Counseling Certification and see if it meets your academic and professional goals
Dealing with postpartum depression can be challenging, but it is important to remember that you are not alone. By understanding postpartum depression, recognizing its impact, and implementing effective strategies, you can navigate this difficult period and empower yourself towards recovery. Whether it’s through self-care, seeking professional help, or building a support system, each step you take brings you closer to healing and embracing the joys of motherhood. Remember to be kind to yourself and reach out for the support you deserve.
Please also review AIHCP’s Grief Counseling Certification and see if it meets your academic and professional goals. The program is online and independent study and open to qualified professionals seeking a four year certification. Licensed professionals in counseling are excellent candidates to earn a Grief Counseling Certification.
Additional Resources
“Postpartum Depression”. HealthEssentials. (2022). Cleveland Clinic. Access here
“Everything You Need to Know About Postpartum Depression: Symptoms, Treatments, and finding help”. Pietrangelo, A. (2022). Healthline. Access here
“Postpartum Depression”. OASH. (2023). Office on Women’s Health. Access here
“Postpartum Depression”. Bruce, D. (2022). WebMD. Access here
Self esteem is critical to an emotional, mental and healthy life. A good self image helps one to live with confidence, approach goals, complete tasks, and find value in oneself. It is essential to find value in oneself and to find oneself worthy of love. Hence cultivating a healthy self esteem is important to a personal, academic, professional and social life.
Low self esteem is an inaccurate self perception with reality. Please also review AIHCP’s Grief Counseling Certification
Self esteem issues can go in two different directions. An inflated self esteem can lead one down an egotistical and narcissistic road with various anti social disorders. It can lead to delusions and foolish endeavors. In essence, it is not in balance with reality. Self esteem can also take an opposite dark road in which one finds no value in oneself and this can lead to depression, loss opportunities, poor health and possible suicide. This article will investigate the later and in particular how one can deal with self esteem and depression.
The article, “How to Manage Low Self-Esteem” by Corey Whelan looks in detail how low self esteem can derail a life, its sources and how to overcome it. She states,
“Everyone has moments of doubt about who they are and what they’ve achieved. You may do or say something that makes you temporarily ashamed of or annoyed with yourself. Those temporary or periodic feelings are not the same as low self-esteem. Low self-esteem refers to long-term negativity about who you are and how you show up in the world. These negative feelings can be persistent and hard to challenge. For example, if someone compliments you, you may not believe them. If you achieve a goal, you may not allow yourself to take credit for it.”
“How to Manage Low Self-Esteem”. Whelan, C. (2022). Healthline.
Causes of low self esteem range from various issues suffered at a younger age. Hyper critical parents or family can damage a child’s development. When a child is unable to meet certain psycho social goals within his/her age the child can be prevented from forming independence and the ability to do things. When a child is shamed for pushing forward, the impulse to be something greater can also be hampered. Hence due to criticism or inability to progress to new stages of development that highlight independence and creativity can greatly affect a child’s self esteem and provide future issues in advancement in life. Other forms of criticism include body shaming and bullying. These type of parental and as well peer abuse can cause severe self image issues within the person.
In addition, many children are unable to form healthy and supportive bonds due to attachment issues with parents. When children are not given security and love, then they become insecure and anxious. They begin to question themselves and find themselves not worthy of love or capable of being loved. These haunting memories of unloved childhood also cause great damage to self esteem.
Trauma and abuse also play a key role in lowering self esteem. Children of abuse, especially sexual abuse, feel dirty and unclean. They feel unable to be loved or love and consider themselves broken. This is often the case because the abuser not only physically assaults the child, but to protect himself/herself creates a illusion within the child’s mind that it is the child’s fault. The child then is haunted and unable to report the abuse and continues to feel broken and dirty.
Untrue Thoughts
Many with low self esteem have a inaccurate self image of self. Either through body shaming or verbal and mental abuse, the person feels they are worthless and amount to nothing. Many feel ugly, or dumb, or unlovable. They hence attach to any form of connection, even if unhealthy. A person with low self esteem is unable to see the value in oneself and is unable to move forward with confidence, accept compliments, boast of achievements, or recognize individual talent within oneself. A person with low self esteem has a difficult time accepting challenges, or attempting harder feats and will surrender before one even tries to do something. A person with low self esteem will feel unworthy, untalented and incapable of great things. Hence, a person will self esteem is unable to take criticism well and will amplify normal comments and make these comments more than what they truly are.
Those with low self esteem have poor self image that is not correlated with truth or reality
A person with low self esteem also has difficulty trusting one’s own instincts. Low self esteems restricts creativity and trust of self to do something. One needs constant coaching or discussion with others to engage in something. Also, low self esteem prevents boundaries. A person with low self esteem has a difficulty saying no to others and will find oneself doing things one does not really want to do. Hence low self esteem turns an individual into a people pleaser instead of looking out for oneself.
Dangerous Road
Those with low self esteem suffer physically, emotionally and mentally. Physically, they tend to take less care of themselves. They feel ugly and feel little need to care for oneself via grooming and exercise. This can lead to un-healthy life styles. Emotionally and mentally, one may punish oneself for false perceptions of being a failure. This can lead to self mutilation, self harm, risky behavior, drug addiction and drinking, depression, suicidal ideation and possible suicide attempts. In addition, it can prevent someone from achieving positive and happy experiences due to fear or rejection. Hence less chance for friendship, love and academic and professional success.
Overcoming Low Self Esteem
It is difficult for someone to overcome self esteem because one is blinded by a false perception. The person lives in a mirage of falsehood. Only till one is opened to reality can one start to escape the dark veil of low self esteem. This takes time, counseling and reframing of self. One can begin to rehabilitate self image through small goals and achievements. Whether it is a hobby, gym work, or academic and professional goals, one can begin to objectively calculate success and find to one’s amazement that these objective successful achievements coincide with not someone else but oneself. Hygiene, personal pride and goal setting can all play key roles in awakening someone to one’s best potential. Counselors can also help those with self esteem with positive affirmations, journaling and finding ways to surround oneself with positive people and energy instead of negative ones.
Overcoming low self esteem when dealing with depression can be an even more difficult feat. Depression already prevents one from finding joy in life. If one already is suffering from low self esteem, one will quickly travel down a darker road. Depression is usually correlated with lower self esteem and can become a result of constant gloomy outlooks on life. Those suffering from low self esteem and depression should constantly look to post positive affirmations about self and try to brag about life. They should write down positive things and journal. They should set realistic goals and avoid comparisons. They should also and most importantly be kind to oneself. Those with low self esteem and depression are their own worst critics. Self love is critical in these cases.
Conclusion
Self image needs to be balanced. It cannot become narcissistic but it cannot become deflated. It needs to find a happy balance with reality that is optimistic and able to help a person reach one’s fullest potential. Unfortunately, many suffer childhood bullying, criticisms and abuse which greatly affects their development and hence self esteem. This can lead to bad physical, emotional and mental health which can develop into possible depression or even suicide. It is important to identify low self esteem find help and incorporate strategies to improve self image. If dealing with depression or other trauma, a licensed counselor can help one find better self image.
Please also review AIHCP’s Grief Counseling Certification
AIHCP also offers a certification in Grief Counseling for qualified professionals in the healthcare and mental healthcare fields. The program is online and independent study and open to qualified professionals seeking a four year certification as a certified Grief Counselor.
Additional Resources
“9 Tips for Strengthening Self-Esteem When You Have Depression”. Coelho, S. (2022). PyschCentral. Access here
“11 Signs of Low Self-Esteem”. Cherry, K. (2023). VeryWellMind. Access here
“Self-esteem: Take steps to feel better about yourself”. Mayo Clinic Staff. (2022). Mayo Clinic. Access here
“Signs of Low Self-Esteem”. WebMed Editorial Contributers. (2022). WedMed. Access here
Dissatisfaction with self and the primal need to eat or not eat are closely tied together. Maslow’s first need is to satisfy hunger and thirst, but while meeting these needs is necessary for existence, other abstract dissatisfactions with self can create mental disorders in fulfilling these needs. A person may deal with depression or great sadness over how he/she physically appears and proceed to great maladaptive approaches to rectify through unhealthy eating habits. Hence due to emotional mindsets, grief, depression and other views of self, one can fall into a variety of different and unhealthy eating disorders. Some may distort their eating habits to produce a certain physical look while others may distort themselves due to an addiction to food during intense grief and depression.
The Body and Eating
The necessity to eat is a need that is closely monitored by the body. When glucose drops, the body and the brain send signals. The hormone, Ghrelin secretes in the stomach to alert the brain of hunger. In addition, the Hypothalamus triggers the hormone Orexin to create the feeling of hunger. Consequentially, the body also reduces hunger through the hormone insulin which reduces sugar in the blood. The body also produces the hormone Leptin from fat cells and when in abundance relates to the brain to increase metabolism.
Depression, bullying, and other self image issues can lead to a variety of eating disorders that go to either extreme of eating too much or not eating hardly at all
Beyond the physiology also is a psychology that surrounds hunger. Individuals have different taste preferences due to experiences and cultural influences, which can create certain pleasures or aversions to certain tastes. In addition when upset, the desire for carbohydrates found in comfort foods increase the neurotransmitter serotonin. When stressed, individuals crave sweets or chocolates to reduce stress. In addition, friends and the one’s environment can also produce needs to eat when one does not really need to eat, as well as serving size and proportions and numerous selections. These stimuli push one to eat things one may regret later or should not eat for health reasons. Hence peer pressure, food selection and availability, previous experiences, as well as emotional moods can all play big roles in how one eats or does not eat.
Over-eating and Obesity
Overeating can be due to depression or even bullying. Individuals may retreat to food and solace to escape the sadness of life. This is commonly associated with the term binge eating. Individuals when they feel bad, may find recourse in eating in great excess or a variety of unhealthy foods. There is usually a deep remorse following binge eating. This maladaptive way to cope with stress or depression while temporarily fulfilling causes more guilt and remorse but also physically is unhealthy. Binge eating is bad for maintaining healthy weight and can be a serious issues with those who suffer from diabetes.
Depression can lead to poor coping through binge eating
Many who suffer from this need to learn better ways to cope with stress, grief and loss. It is important for those who experience higher levels of stress or facing loss to find other ways to express themselves. Better coping strategies can be implementing that are void of food security but help one find relief though healthier outlets such as exercise, hobbies, and activities with friends. Having a friend to call or a person to contact can also be beneficial in removing the psychological temptation to turn to food. Like any addiction, there is a mental crutch that manifests and a false need. Breaking the habit with healthier life styles, other options and a conscious effort is key.
Individuals can shop more healthy, limit portions, eat smaller meals throughout day, and exercise more. The important thing to remember when depressed or addicted to a maladaptive practice, one does lapse. When one does lapse, one needs to be too hard on oneself. A lapse is not a complete collapse and one needs to continue to work towards finding better ways to cope with stress and grief in life.
Anorexia nervosa and Bulimia nervosa
Some individuals deal with stress and loss differently and under eat. Some are bullied about self image through school mates, while others face sharp criticism at home about their appearances. Competition with siblings or friends can lead to a drastic alteration in one’s body and shape through unhealthy and maladaptive eating habits that reduce intake of food for thinner appearances. In Western modern culture, obviously thinner appearance is the desired result but other appearances in other cultures can also be sought after in unhealthy ways as well.
Other than depression, Anorexia is fueled by a poor self image, abuse, extreme perfectionism or OCD
Those seeking a thinner appearance resort to Anorexic behaviors. Starvation diets are implemented due to a false image of being fat. Again due to bullying, competition, criticism, abuse, or depression, individuals will look to control the only thing they can via their appearance. It is again important to note that all cases of anorexia are not due to sexual abuse but can also be due to bullying or competitive and hyper critical families that push a unattainable perfectionism. This leaves a longing within the individual that can never be satisfied leading to maladaptive eating habits that harm the body and strip it of nutrients and growth. Primarily an issue with teens and younger women, the person will either starve oneself or in the case of Bulimia nervosa, eat and then vomit, excessively fast, or utilize laxatives to prevent weight gain. Both Anorexia and Bulimia share a common origin and look to fulfill the same end but through a different strategy.
Conclusion
Eating disorders can be hereditary and psychological. They can be an over indulgence of food or a self imposed starvation. They can stem from abuse, depression, bullying, competition, poor self image, family criticism or a disproportioned perfectionism. They are ineffective ways to cope with stress, loss and grief. Individuals who deal with these issues, regardless of their spectrum, need to find the root cause of their eating disorder and find better ways to cope with the mental issues that are haunting them. Professional licensed counselors can determine the root cause of their eating disorder and help them discover better ways to reduce eating or find self esteem in the way they are.
Whether addiction to eating too much or various mental issues to eat too little, individuals need to learn the root cause of their issues and re-discover healthier eating habits to incorporate into their life. Unhealthy eating in either extreme can have severe long term health consequences. Again, licensed counselors can help individuals better cope with stress or grief or properly understand their core issue that cause an eating disorder. Friends can also help by building up self esteem.
Poor coping and depression can lead to eating disorders. Please also review AIHCP’s Grief Counseling Certification
Obviously discontent, grief and depression can all be causes that lead to a variety of eating disorders. Licensed counselors can also become certified in Grief Counseling and help individuals sort out the grief issue and help them cope better with the loss. Please also review AIHCP’s Grief Counseling Certification and see if it meets your academic and professional goals. The program is online and independent study and open to qualified professionals seeking a four year certification in Grief Counseling.
Reference
“Exploring Psychology” 11th Edition. Myers, D. & Deall, N. (2019). Worth Publishing, NY, NY.
Additional Resources
“Eating Disorders”. (2023). Mayo Clinic. Access here
“6 Common Types of Eating Disorders (and Their Symptoms)”. Petre, A. (2022). Healthline. Access here
“What are Eating Disorders?”. (2023). APA. Access here
“Eating Disorders and Depression”. Grave, R. (2023). Psychology Today. Access here
“Can Depression Lead to Eating Disorders?” Lebow, H. (2022). PsychCentral. Access here