Rogerian and Person Centered Therapy focuses on the client and emphasizes unconditional positive regard and empathy. Please also review AIHCP’s Healthcare Certification Programs
Rogerian and Person Centered Therapy focuses on the client and emphasizes unconditional positive regard and empathy. Please also review AIHCP’s Healthcare Certification Programs
The DSM-V-TR and many psychopathology texts group Somatic and Dissociative disorders together. In the DSM-V-TR somatic disorders are listed after dissociative disorders which are tied to stress and PTSD. They both share created realities that are not true but they also differ in direction. Somatic disorders attach to physical symptoms without no correlating reality or pathology from a physical sense but find their origin in the mind. Likewise, many are tied to anxiety, or fear of possessing the actual disease associated with the symptoms. Dissociate disorders are tied to breaks from reality that do not exist as well but more so in the mind and one’s surroundings. They are tied to trauma and stress. This leads to derealization and depersonalization, various amnesias and dissociative identity stemming from trauma. In this short blog, we will review the basis and criteria of diagnosis for different somatic disorders as well as dissociative disorders.
Please also review AIHCP’s Healthcare Certification Programs, as well as its many Behavioral Health Certifications.
Somatic disorders contain symptoms of a disease created by the mind with no real existence of the disease within the person. Somatic means coming from the mind and manifesting physiological manifestations of a particular physical disorder (Barlow, et, al., 2023). Similar to Somatic Symptom Disorder is Conversion Disorder. Freud believed that the energy associated with mental illness could manifest as physical disease in other parts of the body causing motor control issues that were only a product of the mind (Barlow, et al., 2023).

The biggest difference between Somatic Disorder and Conversion Disorder was the the type of physical manifestation and mental state. In Somatic Disorder there are a broad range of persistent physical disorders including pain and fatigue. These irks and pains cause discomfort throughout the day and lead to intense anxiety within the individual as the person attempts to understand the nature of their illness. Conversion differs in the manifestation and reaction. The manifestation effects motor control and cause paralysis, blindness, or other body movement. It usually follows an immediate stressor and can resolve itself quicker. Hence individuals do not deal with it longer over a chronological period (DSM-V-TR, 2022).
The DSM-V-TR lists these criteria Somatic Symptom Disorder for diagnosis .
A. One or more somatic symptoms that cause significant disruption in life
B. Excessive thoughts or behaviors tied to the somatic symptoms with at least one of the following:
1. disproportionate and persistent thoughts about the seriousness of the issue
2. high levels of anxiety about the symptom or overall health
3. excessive time and energy directed to these symptoms and concerns
C. These symptoms persist for 6 months.
Somatic Symptom Disorder can be specified with predominant pain, persistent symptoms, and as mild, moderate or severe.
(DSM-V-TR, 2022).
The DMS-V-TR lists this criteria for Conversion diagnosis
A. One or more of the symptoms have altered motor or sensory function
B. Clinical findings discover no correlation between the symptoms and recognized neurological disorder
C. There is no rational explanation for the disorder
D. The symptom causes clinically significant distress or functioning
It can be specified as acute, chronic, with psychological or without psychological stressor, with various symptom types such as weakness or paralysis, abnormal movement, swallowing symptoms, speech symptoms, seizures, sensory loss, special sensory loss or mixed symptoms.
(DSM-V-TR, 2022).
Another Somatic related disorder is Illness Anxiety Disorder which deviates from Somatic Symptom Disorder in regards to mild to no symptoms with the fear of disease existing in the mind. In the past it was referred to as Hypochondria (Barlow, et al., 2023). The DSM-V-TR lists the following diagnostic criteria for IAD.
A. Preoccupation with having a serious illness
B. Somatic Symptoms or not present or very mild. Other symptoms related to a different disorder are ignored.
C. High level of anxiety about health
D. The individual performs excessive health related behaviors for checkups
E. Illness preoccupation exceeds 6 months
F. The illness preoccupation has no other mental health disorder explanation
The DSM-V-TR specifies them as either care seeking or care avoidant
Ultimately within all of these disorders, individuals refuse to believe experts and fall more so upon their own anxiety ridden logics. They tend to seek their own information and insist they know more than medical professionals.
Tied closely to this are other disorders resulting in faking symptoms or purposely re-creating the symptoms for medical help or attention. Some do this for mental reasons, while others seek financial reward via malingering. Obviously those who seek medical attention and cause symptoms for no logical or financial reason suffer a deeper issue. Factitious Disorder results in this deception to gain attention or aid. Some may also look to keep attention on a person under one’s care by causing or lying about symptoms. In the past this was referred to as Munchausen Syndrome (Barlow, et al., 2023).
It is interesting to see the power of the mind to cause physiological symptoms. Yet if one simply realizes the power of worry to cause a stomach ache, then one can see on a large scale how somatic symptoms can manifest in individuals with greater anxiety and distorted beliefs about health.

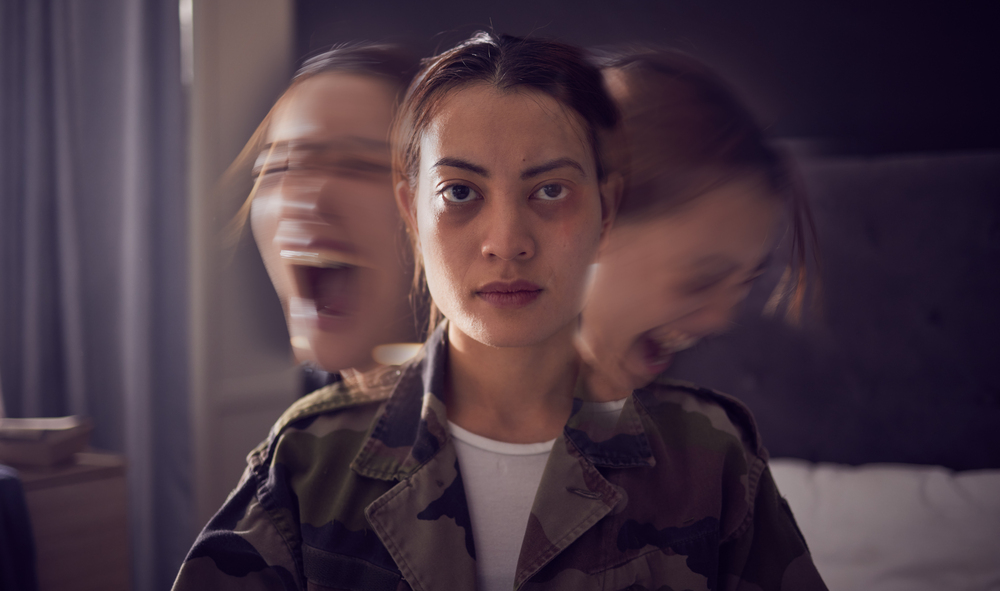
While the mind can create physiological symptoms, it can also create separations from reality due to traumatic events or high levels of stress. Many of the dissociative disorders are closely tied to PTSD and trauma induced orders and directly follow the DSM-V-TR’s chapter on Trauma and Stress Related Disorders. The DSM-V-TR points out that many dissociative disorders are frequently in the aftermath of severe trauma. Their symptoms include “unbidden intrusions into awareness and behavior, with accompanying losses of continuity in subjective experiences (2022). This leads to depersonalization, derealization, amnesia and dissociative identity. They can all play roles in the more general umbrella of PTSD but also be a diagnosis within itself.
Depersonalization/Derealization Disorder
According to the DSM-V-TR, depersonalization is the experience of unreality, detachment or being outside or external from one’s own thoughts, or feelings or even sensations of the body. One senses a distorted senses of time and feels absent from self as if almost outside of one’s own body (2022). Similar and also shared frequently between the two is the subjective experience of derealization. Within derealization one experiences unreality and detachment from one’s surroundings as if reality is dreamlike or foggy or distorted (2022).
Dissociative Amnesia
Loss of memory due to trauma leaves the person with an inability to recall or remember. The loss of memory can be localized or selective only to the event, or in more severe cases generalized and effecting one’s identity (DSM-V-TR, 2022). In some cases, it can be specified with dissociative fugue where the individual travels or wanders and cannot relate where they came from (2022).
Dissociative Identity

One of the most wild and bizarre forms of dissociation is multiple personalities. The DSM-V-TR now labels it as Dissociative Identity in which the person creates different identities when faced with intense trauma. These identities are formed at a younger age and usually add new ones as the person needs to adjust to the unresolved trauma. The DSM-V-TR lists the following criteria for diagnosis
A. Disruption of identity by two or more distinct personality states. The disruption marks a distinct discontinuity in sense of self which displays changes in behavior, memory, perception, consciousness, cognition and sensory-motor functioning.
B. Recurrent gaps to recall events and personal information are inconsistent with normal forgetfulness
C. The symptoms cause significant distress to all elements of social functioning
D. The disturbance is not part of a cultural or religious practice
E. The disturbance is not associated with other substances or medical conditions
(DSM-V-TR, 2022).
Barlow states that most experience an average of 15 different personalities or alters. These alters merge from the host identity (2023). It is believed that under severe cases of trauma, younger children who may possess a genetic and biological vulnerability can develop DID. Diagnosing DID should be done with great care as not to lead an individual to bias or place falsememories regarding a person’s past. Ultimately, it is very difficult to fake DID although criminals in the past have attempted to use a DID defense (Barlow, et, al. 2023).
Some identities are classified as possessive identities which can be mistaken for demonic manifestation. If existing within the religious traditions, one must be careful of cultural and religious beliefs regarding this. In fact, the Catholic Church goes to great lengths and diagnosis within itself to determine a difference between a possessing identity with what it considers to be an external source in its manual of exorcism. Obviously before the era of modern science, many DID were considered possessions and did not meet the current diagnosis within the Catholic Church. Those who are not religious still doubt any form of possession within itself but that is a debate for another day.
Physiological symptoms can be very real. The brain can shut itself off for its own defense and create different realities. These are all things that modern psychology has discovered. Many of these issues stem from trauma, anxiety and stress. When a person has the biological vulnerability, the recipe for the manifestation for these disorders become a reality for the person. Therapy and medication can play large roles in facing past issues and traumas. With the exception of DID, many of these mental issues can resolve quickly with proper care. Obviously DID deals with a far deeper trauma and requires deeper psychotherapy to unify the person. That involves identifying triggers, reliving trauma, and carefully realigning the past without causing more damage (Barlow, et al., 2023).
Please also review AIHCP’s Behavioral Health Certifications. AIHCP offers Trauma Informed Care as well for professionals seeking additional training and credentials in this field.
Disruptive and Impulse Control Disorders. Access here
Personality Disorders. Access here
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorder” DSM-5-TR (5th ed., text revision). American Psychiatric Association Publishing.
Barlow, D.H., Durand, V.M., & Hofmann, S.G. (2023). Psychopathology. An integrative approach to mental disorder (9th ed.). Cengage Learning
Goodman, B. 2024. “Somatic Symptom and Related Disorders”. WEBMED. Access here
“What is Somatic Symptom Disorder?” APA. Access here
“Dissociative Identity Disorder (Multiple Personality Disorder)” (2024). Cleveland Clinic. Access here
“Dissociative Identity Disorder (Multiple Personality Disorder)”. PsychologyToday. Access here
CBT is a behavioral grounded therapy that helps correct distorted thinking. Developed by Beck and Ellis it has proven to be a powerful tool in correcting bad thinking and transforming negative beliefs. Please also review AIHCP’s Healthcare Certifications
Emotional loss of control that translates into disruptions, conduct violations against social norms and laws, and the rights of others are the product of a variety of deeper seeding issues stemming in childhood. While many of these disruptive, impulse control and conduct disorders manifest in early childhood, if left unchecked, they can continue to develop into early adulthood and root into a person’s personality. In fact, conduct disorder itself, can be a precursor to anti-social disorder (DSM-V-TR, 2022). With this in mind, it is important to teach, guide and when necessary reprimand children in accordance with morality, authority and law. This is especially true for individuals who genetically have a predisposition to impulse control, emotional outbreaks and defiance.

Please also review AIHCP’s behavioral health certifications, including Anger Management Courses, as well as ADHD Consulting.
These types of disorders include issues with emotional control but especially when it infringes upon the rights of others.
Oppositional Defiant Disorder
This disorder tends to manifest early in childhood but can continue to persist in adulthood and hamper a person’s future relationships as well as one’s interaction with authority figures. The DSM-V-TR points out that it is marked with a pattern of an overall angry and irritable mood that displays itself in an argumentative, defiant way, characterizing vindictiveness. This mood persists for at least 6 months (DSM-V-TR, 2022). It is important to evaluate this time frame because child development can sometimes mimic these behaviors short term and not necessarily constitute a long term disorder. During this 6 month period, the individual must exhibit four of the below symptoms with at least one person who is not a sibling.
1.losing temper
2. touch or easily annoyed
3. often angry or resentful
4. often argues with authority figure
5. defies or refuses to comply with requests from an authority figure
6. deliberately annoys others
7. blames other for his or her mistakes or behaviors
8. exhibited spitefulness or vindictive behavior twice within the last 6 months
These symptoms can be specified as mild, moderate or severe (DSM. V-TR, 2022).
Intermittent Explosive Disorder
Loss of control and temporary rage can sometimes be more than a mere temper, loss of patience, or anger issue but can also be an emotional disorder that requires deeper care and therapy. Intermittent Explosive Disorder emerges in childhood but can also persist into adulthood and cause serious relationship issues in all aspects of life and especially result in criminal charges. The DSM-V-TR cites that IED exhibits frequent and recurrent outbursts due to a failure to control aggressive impulses (2022). These outbursts can result in verbal aggression including temper tantrums, tirades, verbal arguments or even physical aggression towards property, animals or other people. The outbursts can be limited to only verbal but also to physical confrontations that cause damage and injury. The DSM-V-TR states that 3 serious infractions must occur within a 12 month period that result in damage or destruction, but frequent verbal aggression according to the first standard meets the first criteria.

In addition to verbal or physical outbursts, the magnitude of the aggressiveness must not be proportionate with the provocation or to any of the causing stressors. Individuals with IED react completely out of proportion to life events and daily stresses that others would not react to (DSM-V-TR, 2022). In addition, these outbursts are not premeditated or meant to achieve some objective but are purely reactive. In addition, these recurrent aggressions and outbursts cause considerable impairment to the person’s personal, professional, and interpersonal functioning. Finally, the person must be at least 6 years of age. This disorder manifests at a higher level in males and exist in both children and adults if left untreated (DSM-V-TR, 2022). Please also review AIHCP’s Anger Management Consulting Certification.
Conduct Disorder
Conduct Disorder is a repetitive and persistent pattern of behavior which violates the rights of others, social norms and rules and laws of societal norms (DSM-V-TR, 2022). If 3 of the following 15 criteria is met over the past 12 months, with one having to be within 6 months, then an individual may be diagnosed with Conduct Disorder. The categories of disorder include aggression, destruction of property, deceitfulness and theft, and serious violation of rules.
The DSM-V-TR points out that these acts constitute great inter-social impairment and have occurred before 18. If over 18, the individual can qualify for diagnosis of Anti-Social Personality Disorder (2022). Specifiers include childhood onset and adolescent onset. In addition, specification can include with limited prosocial emotions, lack of remorse or guilt, callous or lack of empathy, unconcerned about performance, and shallow deficient affect (DSM-V-TR, 2022). The condition can finally also be classified as mild, moderate or severe.
Within Conduct Disorder as well as Anti-Social Disorder, two other types of disorders can manifest.
Pyromania
This disorder leads to the deliberate and purposeful choice to set fires on more than one occasion. The DSM-V-TR differentiates the setting of fire for reason or gain to that correlated with an affective arousal before the act that includes a fascination or interest about the attraction to fire. Pleasure, gratification or relief is associated with setting the fire (2022).
Kleptomania
Like fire setting, the act of stealing in Kleptomania is not tied to gain or need but a recurrent failure to resist the impulse to steal due to the sense of tension to commit theft. From this theft, comes gratification and relief that is not associated with any motive or need (DSM-V-TR, 2022).
ADHD is not listed with these types of disorders in the DSM-V-TR but is listed under neurodevelopmental disorders, but it does cross lines with many impulse disorders and is commonly comorbid with those who also possess them (DSM-V-TR, 2022. Obviously man individuals with ADHD are not criminals, or have rage, but symptoms of ADHD can contribute to the inner turmoil of those. This may have something to do with the lack of control of impulses and constant inability to maintain focus on one thing.

For purposes of analysis, the DSM-V-TR states that ADHD causes persistent lack of ability to focus attention and/or possess hyperactivity or impulsiveness in behavior. Some may exhibit only inattentiveness, while others may just display hyperactivity, while some may be burdened with both sets of symptoms. These symptoms emerge before age 12 and can persist into adulthood. Some elements of it are later controlled by a more developed brain in adulthood and manifest in other ways. Inattentive symptoms include at least 6 of the following over a 12 month span
Hyperactive symptoms must include 6 of the following over a 12 month period
Again, according to the DSM-V-TR, these symptoms can be predominantly inattentive or hyperactive or consist of both symptoms. It can also be classified as mild, moderate or severe (DSM-V-TR, 2022). It is no wonder then that many of these issues also correlate with various disruptive, impulse control and conduct disorders or later can possible develop into it. Please also review AIHCP’s ADHD Consulting Program.
Many of these disorders include both nature and nurture. ADHD exists at a level of 4 to 5 percent worldwide within children (Barlow, et al., 2023). Genetically, individuals can be prone to higher risk taking within the brain that inhibits fear or punishment (Barlow, et al,.2023). Biologically, levels of serotonin and epinephrine can be low with higher levels of testosterone (McRay, et al, 2016),. In addition, lack of family discipline, family dysfunction, divorce, and lack of family involvement can lead to deeper seeded issues that manifest in the child’s behavior and if not treated later manifest in adulthood (McRay, et al., 2016).
Treatment for conduct and impulse control issues include behavioral strategies that try to correct the operant conditioning previously experienced in life. Others include training for parents to better manage the child and teach the child structure. Also important, includes various forms of CBT that look to help empower the child with better social cognition skills and problem solving strategies. For anger issues, sometimes peer groups can help. Anger Management skills can help many find solutions to their temper. Finally, stimulant medication can be beneficial due to these disorders high comorbidity with ADHD (McRay, et al., 2016).
Ultimately, disorders are not justifications for poor behaviors but they are explanations why some children, and even adults, are more inclined to react and behave certain ways. Merely because someone feels an urge or a stronger intense feeling to do wrong or be cruel is never a justification but with therapy and sometimes medication, individuals can be taught to better control and maintain disruptive and impulse control behaviors.
A strong moral conviction of right and wrong is always a powerful deterrent in life. Understanding within one’s conscience that a feeling or urge does not justify a certain behavior is the first step to finding the help one needs. Obviously at an earlier age, parental guidance and discipline is essential to prevent these disorders from completely transforming an individuals personality into habitual chaos. Anger, lack of impulse control, defiance of authority and rage lead to many crimes and broken lives. It is hence important to maintain control in these situations and if one cannot to find the necessary guidance and help to learn how to control one’s inner disorders.
Please also review AIHCP’s Behavioral Health Certifications as well as AIHCP’s Anger Management Consulting Certification as well as its ADHD Consulting Program
Intermittent Explosive Disorder. Access here
ADHD. Access here
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorder” DSM-5-TR (5th ed., text revision). American Psychiatric Association Publishing.
Barlow, D.H., Durand, V.M., & Hofmann, S.G. (2023). Psychopathology. An integrative approach to mental disorder (9th ed.). Cengage Learning
McRay, B.W., Yarhouse, M.A., Butman, R.E., & Kiple, C. (2016). Modern psychopathologies: A comprehensive Christian appraisal. (2nd, ed.) IVP Academic
“What are Disruptive, Impulse Control and Conduct Disorders?” APA. Access here
IED. Mayo Clinic. Access here
ODD. (2026). Cleveland Clinic. Access here
“Oppositional Defiant Disorder”. Psychology Today. Access here
Bhandari, MD, (2024). “Mental Health and Conduct Disorder”. WebMD. Access here
Personality Disorders are one of the more interesting types of disorders in mental health. They attract the most attention and curiosity about why individuals act the way they do. For the secular mind, it attempts to explain right and wrong, criminality, oddities, and other quirks that step out of bounds within the social structure. As observed in early psychology, it a disorder but the mind still has the ability to possess rationale in its own self. From a religious perspective, it constitutes the reality of brokenness of humanity and how individual acts of deviation can become habitual aspects of one’s personality (McRay, 2016). These disorders distort personality to such an extent to cause inner personal turmoil in one’s feelings towards others and one’s assertion of those feelings outside the norms of one’s cultural context (McRay, 2016). For this reason, many personality orders are not only odd, eccentric, selfish, rude, and withdrawn, but also violent and terrifying to others.
Personality in itself is an essential feature to a person. It involves a person’s overall demeanor, it includes how a person reacts internally and externally with others and the person’s overall temperament. Overall, a personality is one’s unique patterns of thinking, acting and feeling (Myers, 2019). There are numerous theories of personality ranging from the psycho-analytic schools to the humanistic as well as the behavioral schools of psychotherapy. All emphasize their targeted areas of study to the development of personality and all add unique elements to understanding personality. Within personality, exist various traits that are essential to proper functioning within the norms of society. Traits are characteristics or behaviors or dispositions of how a person feels or acts in certain ways (Myers, 2019). Experts list the Big Five Factors of traits that determine personality factors. Myers lists Conscientiousness, Agreeableness, Neuroticism, Openness and Extraversion (2019). When one sways from one extreme to the other in these traits, then imbalance occurs. In addition, the DSM-V-TR also lists these traits in its alternate diagnosis for personality disorder with openness being replaced with lucidity (2022).
When an individual deviates from the cultural norms of his or her culture and society and these extremes manifest against the core basic traits, one will witness odd or deviated social behavior, but isolated acts of misconduct or erratic behavior do not constitute a disorder. A disorder is far more deeper and its duration long lasting. In this blog, we will take a closer look at personality disorders and their striking deviations from cultural norms and behavior.
Please also review AIHCP’s Healthcare and Behavioral Healthcare Certifications
The DSM-V-TR points out that an enduring pattern of inner experience and behavior that deviates from expectations of one’s culture constitutes a personality disorder. These disorders manifest in one or two ways, via cognition, affectivity, interpersonal functioning or impulse control. The DSM-V-TR continues that these enduring patterns are inflexible and pervasive across the range of the person’s personal and social situations and interactions with others (2022). The DSM-V-TR states that these behaviors cause significant distress and impairment in social and personal relationships and this pattern remains stable and of long duration with origins in adolescence and early adulthood (2022). Obviously, these issues are not related to substance abuse, medication, or other mental defects.
The DSM-V-TR looks at moderate to severe impairment in traits to affect identity, self-direction, empathy and intimacy. In addition, these disorders can portray various distortions of personality traits to the extreme. They can manifest negative affectivity versus emotional stability, detachment versus extraversion, antagonism versus agreeableness, disinhibition versus conscientiousness, and psychoticism versus lucidity (2022). It is because of this one can witness in personality disorders a wide range of odd, eccentric, emotional, impulsive, egocentric, aggressive, violent, unempathetic, and manipulative traits.
The DSM-V-TR groups personality disorders into three clusters. Cluster A includes paranoid disorders such as paranoid, schizoid and schizotypal. Cluster B includes personality disorders such as anti-social (sociopathy/psychopathy), borderline personality disorder, histrionic, and narcissistic disorders. Finally, Cluster C includes avoidant personality disorders such as avoidant, dependent and obsessive compulsive personality disorders (not to be confused the OCD itself). (2022).
Of particular note, based on different case studies and surveys, the percentage of personality disorders within the general population is 9 to 10 percent suffering from some type of personality disorder in some degree or level (Barlow, et al. 2023). Ironically, many of the terms associated with these disorders, are used loosely in everyday vernacular towards individuals who may act a certain way in a given situation but not possess the disorder. Bad behavior, sin, vice, or whatever one wishes to label it is part of the human condition and people are not perfect. Personality Disorders are merely a persistent form of these behaviors at an extreme and rigid level. So, when diagnosing, anyone at some time or some point can see at least a couple undesirable traits and feel guilt or shame for exhibiting these actions. Ultimately guilt and shame and acknowledgement are key signs one does not possess the disorder itself.

Paranoid
Paranoid personality disorders are in the realm of psychotic and the schizotypal form can sometimes be the premorbid phase of schizophrenia itself. One of the key elements is the disorder is persistent before and after any delusional of psychotic episodes.
Paranoid Personality Disorder constitutes a pervasive distrust and suspicion of others. Without evidence, they feel they are being exploited or harmed. They discover unfounded evidence of demeaning actions or threatening meanings in other individual’s remarks or cues. They are preoccupied with doubts of other’s loyalty to them and find it difficult to confide in others. They feel information can constantly be used against them. Emotionally, they can become angry and hold grudges due to the perceived threats (DSM-V-TR, 2022).
Schizoid Personality Disorder is a detachment from social relationships beyond intimate family. They also possess a restricted range of emotions. These traits continue before and after remission of possible psychotic episodes (DSM-V-TR, 2022). Schizotypal Personality Disorder is more severe and resembles Schizophrenia and other schizophrenic spectrums. It can also co-exist with them but also exists outside the psychotic psychotic episodes (2022).
Anti-Social
Anti-Social Personality Disorder is best known a pervasive and consistent pattern of disregard and violation of the rights of others, occurring since age 15 and must be at least 18 (DSM-V-TR, 2022). With diagnosis, three of the following traits must persist

The DSM-V-TR continues in alternative diagnosis with emphasis on a distorted identity based on egocentrism and self-esteem deprived via power and gain and pleasure. Personal gratification is the primary goal and self direction absence of inhibitions that prevent those gratifications. There is a lack of emotional connection or empathy within the disordered person and intimacy and relationships are meant for exploitation or manipulation to meet one’s own needs. The DSM-V-TR in addition lists these traits of which 6 must be met
Horrifying enough, there can be a psychotic specifier as well with psychopathic features which would constitute the differences between a sociopath and a psychopath. Depending on degree and opportunity, these individuals can be very dangerous in what they are willing or not willing to do to others. Many criminals possess these traits and those in trouble with the law. Many can understand something is wrong but fail to care or display empathy or guilt or emotion regarding their actions.
Narcissistic Personality Disorder is commonly comorbid with Anti-Social Personality Disorder. Narcissists, according to the DSM-V-TR, display a pattern of grandiosity. They require admiration and lack empathy. The disorder can manifest in early adulthood (2022). Five or more of the following are necessary for diagnosis.
In regards to identity, they require excessive reference of others for self-definition. Deep down, they have lower self-esteems and without these appraisals, they can suffer emotionally. In addition, self direction is tied to gaining approval of others. Relationships and intimacy are more superficial as to the image it portrays. Empathetically, they are restricted in understanding the needs and emotions of others at the expense of their own (DSM-V-TR, 2022). Closely related is Histrionic Personality Disorder which faces excessive emotionality and seeking of attention (DSM-V-TR, 2022).
If the other anti-social disorders are more intellectual, then Border Line Personality Disorder (BPD) is the chaos of emotion. According to the DSM-V-TR, BPD is a pervasive pattern of instability in regards to relationships, self-image and affects which onsets in early adulthood (2022). Five or more attributes must be present.
In regards to identity, BPD is marked by poorly developed and unstable self-image. Self direction consists of instability with goals and plans. Empathetically, individuals have a difficult time recognizing the feelings and needs of others. In regards to intimacy and relationships, there is a consistent intense, unstable and constant conflict with others (DSM-V-TR, 2022). They experience intense emotional lability, anxiousness, separation insecurity, depression, impulsiveness, risks and hostility (DSM-V-TR, 2022).
Avoidant

Avoidant personality disorders include Avoidant Personality Disorder, Dependent Personality Disorder and Obsessive Compulsive Personality Disorder.
Avoidant Personality Disorder involves more than an introvert life style or bouts with anxiety but a pervasive pattern of social inhibition, inadequacy, and hypersensitivity to negative evaluations of self (DSM-V-TR, 2022). Four or more of the following are need in diagnosis.
Avoidant personalities are associated with low self esteem identity wise. Their self direction is distorted due to reluctance to pursue goals. Their empathy for others is distracted by their own internal fears and their intimacy is restricted due to shame and fear of rejection. Their traits include anxiousness, withdrawal, anhedonia and intimacy avoidance (DSM-V-TR, 2022).
Dependent Personality Disorder involves a pervasive or excessive need to be taken care of by others which leads to submission and clinging behaviors marked by separation anxiety which manifests in early adulthood (DSM-V-TR, 2022). Five or more of the following symptoms are required for diagnosis.
Finally, Obsessive Compulsive Personality Disorder concludes the avoidant disorders. This disorder is not to be confused with OCD which can be comorbid but unlike OCD which reacts to stressors and anxiety, OCPD exists in all situational relationships. According to the DSM-V-TR, it is represented by a pervasive pattern of preoccupation with order, perfection and mental and interpersonal control at the expense of flexibility which begins in early adulthood (2022). Four or more of the following symptoms are necessary for diagnosis
Those with OCPD compose their identity as correlated with work or productivity. Their self direction is complicated due to rigidity in completing tasks and meeting standards. They lack difficulty in empathy to understand the feelings and standards of others. Finally, their intimacy is restricted in relationships since they put relationships secondary to work and maintain a rigid and stubborn life with others (DSM-V-TR, 2022). They adhere to rigid perfectionism, perseveration in tasks, intimacy avoidance, and possess restricted affectivity (DSM-V-TR, 2022).

Personality Disorders like all mental pathologies cannot be originated from one aspect of life but is a culmination of biological, genetic, psychological, behavioral and social factors. In addition, many possess comorbid mood disorders or maladaptive coping strategies involving substances. In the cases of Anti-Social Personality, it is obvious that there are genetic dispositions as well as biological deformities within the brain that restrict empathy and impulsivity (Barlow, et al., 2023). In addition, early childhood mistreatment, abuse, trauma, poverty and malnutrition can play roles in the development of life views and emotional affectivity (McRay, 2016). None of these things guarantee a disorder, but they collectively can contribute to disorders that later develop in early adulthood.
In children, values and morality are also essential to enforce in life. In early development of a children, egocentrism is important to survival but children are exposed to empathy, love and the needs of others. Children that are not properly guided can develop vices that later can lead to habitual life styles (McRay, 2016). Children with natural inclinations to pride, or selfishness, or other vices, without the proper guidance can fall victim to these inclinations as adolescence continues. These maladaptive behaviors manifest as the person is permitted without consequence to perform these actions. Obviously from a religious perspective, morality and restrictions are essential guardrails in anti-social personality development (McRay, 2016). Even without proper social norms and concepts such as the Golden Rule, individuals can develop into habitual disordered individuals in mind, thought, emotion and behavior.
Unfortunately, many individuals with personality disorders do not seek treatment. Avoidant groups are the most likely to seek help but anti-social and paranoid seek assistance less. Those who do find help require extensive and consistent counseling that focuses on emotional regulation, identifying distorted thinking, and understanding the needs of others. This involves comprehensive psychotherapy that includes CBT, DBT and other cognitive therapies. Humanistic therapies can attempt to at least encourage acknowledgement of the needs of others. Medication is rarely helpful but only to alleviate secondary symptoms of anxiety or depression, especially in BPD (Barlow, et al., 2023).
Pastoral and Christian Counseling care has existed well before modern psychology. In these practices, the proposed opposite virtue of the habitual vice was emphasized such as humility over pride or temperance over anger. In these cases, the spiritual treatment of the sinful condition was considered in addition to the mental pathology. Moral virtues, spiritual discipline, submission to God and constant regulation over viceful responses were considered critical. For many, faith left the change to the grace of God due to the sinful nature of humanity(McRay, 2016).Too many times, pastoral leaders or even counselors and mental healthcare professionals can become over involved in personality disorder cases looking to rescue and save these clients. Many of these clients unfortunately are sometimes beyond saving and will attempt to manipulate helpers.
In regards to loved ones, family is encouraged to never withdraw love but to always protect themselves from manipulation or abuse. In addition, they are to set strong boundaries with those facing personality disorders. Boundaries are essential and must be made clear and definitive of expectations but also demands for treatment. Family needs to become psycho-educated on the disorders and be able to identify manipulations or emotional states to better protect themselves but also help the person.

Personality Disorders are habitual, persistent, and impairing traits that affect an individual’s ability to show empathy, regulate emotion, or interact with other people in a fair and just way. The disorders affect their ability to properly assert themselves in positive or negative ways. They manifest in types or paranoid, anti-social or avoidant. All individuals to some extent sometimes deviate from the norm or do something wrong, but personality disorders deviate from the cultural norm on a consistent basis and at disproportionate extreme. While those who suffer from these disorders, especially BPD and Sociopathy must be held accountable for bad actions, one still must understand the unnatural impulse that has habitually sidetracked their ability to operate as normal individuals. This leads to erratic, odd, distant, dysregulated, manipulative, rigid, emotional, or dangerous behaviors. These disorders have multiple origins from genetics, biology, as well as past trauma, and behavioral upbringing. It is difficult to predict what factors will lead to a true disorder but roughly 10 percent of the population suffers from a personality disorder. In regards to treatment, psychopathology and some medications can help alleviate anxiety and depression, but overall, a person must commit to life long therapy and continually identify their issues. Ironically, the inability to acknowledge this is the biggest issue for adjustment. Finally, it is important to form healthy boundaries with loved ones who suffer from these disorders. While many are hard to understand or even tolerate, it is important to remember they are broken. This does not mean one surrenders oneself to their desires, nor does it mean one justifies their actions or does not hold one accountable, but it does demand an empathetic condition for their brokenness.
Please also review AIHCP’s Healthcare Certification Programs and see if they meet your academic and professional goals.
Anti-Social Disorders – Access here
Narcissism Video- Access here
Borderline Personality Disorder- Access here
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorder” DSM-5-TR (5th ed., text revision). American Psychiatric Association Publishing.
Barlow, D.H., Durand, V.M., & Hofmann, S.G. (2023). Psychopathology. An integrative approach to mental disorder (9th ed.). Cengage Learning
McRay, B.W., Yarhouse, M.A., Butman, R.E., & Kiple, C. (2016). Modern psychopathologies: A comprehensive Christian appraisal. (2nd, ed.) IVP Academic
Personality Disorders. Cleveland Clinic. Access here
Burton, A. (2024). “The 10 Personality Disorders”. Psychology Today. Access here
Personality Disorders. Mayo Clinic. Access here
Pugle, M. (2026). “10 Types of Personality Disorders”. Very Well Health. Access here
When personality disorders compound, some very disturbing types of individuals can emerge. This video looks at the Dark Triad and the dark disorders it encompasses within the Anti-Social spectrum of disorders. Please also review AIHCP’s numerous mental health certification programs
When one considers the classical image of mental illness, psychosis, hallucinations and delusions are the first to come to mind. This can create frightening images or archetypes, or remind individuals of the old asylums of the late 19th and early 20th centuries. While some of the symptoms of psychosis and schizophrenia can be odd and frightening to some, the reality is most are individuals who are suffering and trying to survive. 1 in 100 individuals suffer from schizophrenia and if exists within family history , the chances of inheriting the gene that activates it rises (McRay, et al., 2016). With that in mind, more individuals than one would think suffer at some level within the spectrum of Schizophrenia and psychosis related disorders. This blog will review the DSM-V-TR and its diagnosis of Schizophrenia as well as related disorders.
Please also review AIHCP’s Healthcare Certifications for behavioral health professionals, as well as nurses and other healthcare professionals.
Psychosis itself can occur within any hallucinating drug, substance or meditation. Those with the genetic predisposition can activate it in life by use of drugs, or enduring various stressors (McRay, et al., 2016). The disorders have no gender bias and usually occur late in adolescence or early adulthood (Barlow, et al., 2023). The first phase consists premorbid conditions of cognitive and social impairments, followed by the prodromal phase which exhibits minor psychotic like behaviors for 1 to 2 years. It can take up to 10 years for one to fully manifest positive and negative symptoms with the deterioration continuing without treatment (Barlow, et al., 2023).
Since Schizophrenia is highly connected to family history, various neurological defects are apparent, including larger ventricles, as well as higher levels of the neurotransmitter dopamine (Barlow, et al., 2023). For some, the use of drugs, as well as stressors can play a role in activating it. Finally, fetal exposition to viral infection and different pregnancy complications can play a role (Barlow, et al., 2023).
There is not merely one type of psychosis, but a full spectrum that illustrates Schizophrenia and psychosis and how it manifests differently at various degrees and durations. The DSM-V-TR lists the spectrum as consisting of Delusional Disorder, Brief Psychotic Disorder, Schizophreniform Disorder, Schizophrenia, Schizoaffective Disorder, and Psychotic Disorder due to Substance or Medication induced. Schizotypal Disorder is briefly listed but categorized within personality disorders (DSM-V-TR, 2022).
Within all of these disorders to some extent or level certain symptoms manifest in extremity, duration or presence that are key in differentiating one disorder from another, but within that group of symptoms are clear signs that point to some type of psychosis. Within the nature of psychosis delusions, hallucinations, negative symptoms and disordered speech and thought are key divisions of psychosis.
Delusions

Delusions are a disorder of thought content (Barlow, et al., 2023). The DSM-V-TR adds that delusions are unable to change or be altered even if conflicting evidence against them is supplied to the person (2023). Persecutory delusions are beliefs that an individual is being persecuted, or that one is going be harmed or harassed by a group. Individuals who feel the CIA or FBI is hunting them is a prime example of this type of delusion. Referential delusions are when the individual believes that certain benign cues, gestures, or comments are directed at them. Grandiose delusions refer to delusions that entail the person thinking he or she is someone famous or has individual powers not possessed. Erotomanic delusions entail belief that someone is in love with them, even someone famous. Nihilistic delusions are strong convictions that a catastrophe will occur and finally Somatic delusions are fears regarding health and organ functioing (DSM-V-TR, 2023). Furthermore delusions are considered bizarre if the delusion falls out of the category of even possible, such as aliens inserting a chip in someone’s head (DSM-V-TR, 2023). It is important to differentiate strongly held beliefs or convictions from delusions as well as culturally based ideals that may seem odd to others.
Hallucinations
Hallucinations are perception like experiences that occur without external stimulus (DSM-V-TR, 2023). They can be auditory or visual and must occur within the range of normal experiences. The most common hallucination in Schizophrenia is auditory. Interesting to note, that when individuals experience auditory hallucinations, it the area of the brain associated with speech or Broca’s area that has been shown in experiments to activate instead of the hearing area known as Wernicke’s area. This is because the voices are actually coming from own’s speech area and not from a true external auditory source (Barlow, et. al. 2023).
Those from other cultures or religious traditions, especially within mysticism, are not always considered to be hallucinating. The DSM-V-TR clearly specifies that these cases need to be evaluated differently than a pure disorder (2023). Apparitions and voices of a deity should be evaluated to rule out any mental defect but in some cases no defect exists. Sometimes, a religious experience can possess qualities of a hallucination but the information or message is foreign from the person. Other times, religious experiences can affect the five senses themselves and are not hallucinations. It is important for any spiritual message to sometimes undergo rigid investigation to understand if it is from within a person or if filtered into the person through a spiritual source. Ultimately, how one views these experiences will pend on if one is an atheist or a believer in the spiritual realm. Regardless, they deserve special differential treatment in diagnosis than pure hallucinations before denying it or labeling one with a disorder.
Disorganized Thinking, Speech and Abnormal Motor Control
It is common with psychosis and schizophrenia for many odd cognitive thoughts, reactions, and word salads to emerge within the individual. This is part of the disorder and inability to process thoughts and reality. The DSM-V-TR lists a variety of disorganized thinking and speech symptoms, including derailment or loose association where the person switches without logic from topic to topic, or tangentialtions that illustrate completely unrelated answers to questions. In addition, incoherence can reach such a state where a word salad manifests where the train of thought is impossible to follow (2023). In other cases, inappropriate affect can emerge in which the person’s emotional responses do not match the question or situation (Barlow, et. al., 2022).
In regards to motor control, some individuals display catotonia or decreased ability to react to stimuli. It can also manifest in incomplete or no verbal responses such as stupor or mutism. It is important to note that catatonia symptoms while related to schizophrenia exist, they can also exist in other disorders as well (DSM-V-TR, 2023).
Negative Symptoms

Positive symptoms such as hallucinations and delusions are directly manifested in psychosis and schizophrenia, but there are also passive or negative symptoms. Among them are avolition, alogia, anhedonia, asociality, and affective flattening (Barlow, et al., 2022). Avolition deals with inability or interest to partake in daily tasks. Alogia refers to the absence of speech. Anhedonia refers to the indifference to pleasure or activities that are a source of pleasure. Asociality refers to withdraw and lack of interest of social interaction. Finally, affective flattening is a lack of emotional response or a flat affect to questions or a situation (Barlow, et al., 2022).
Delusional Disorder
This disorder requires the presence of at least one type of delusion for the persistence of one month and the delusions must cause social impairments but do not appear as bizarre or as odd of those exhibiting schizophrenia. These delusions are not due to drugs, substance or other medications and finally, Hallucinations, negative symptoms and disorganization is rare and any form of catatonia rules out this diagnosis (DSM-V-TR, 2022).
Brief Psychotic Disorder

A brief psychotic disorder exhibits the positive symptoms and is not described by other mental health issues such as major depression or bi-polar. It lasts a minimum of 1 day to 1 full month and then a full return to premorbid level of functioning (DSM-V-TR, 2022).
Schizophreniform
This disorder possesses all the positive and negative symptoms of schizophrenia but its duration is its key attribute. It manifests from 1 month to 6 months (DSM-V-TR, 2022). It is also not attributed to any other mood disorders or drugs, substances or medications.
Schizophrenia
Schizophrenia requires 2 of the following during a period exceeding 1 month.
1.delusions
2. hallucinations
3. disorganized speech
4. grossly disorganized behavior
5. negative symptoms.
Of the above conditions, one must be from delusions, hallucinations or disorganized speech.
In addition to these core psychosis symptoms, there must be significant impairment and functioning with work, social interaction and self care. These signs must persist beyond 6 months. In addition, major depressive disorder and bi-polar disorder must be ruled out. Finally, the disorder must not be due to any drug, substance or medicine. (DSM-V-TR, 2022).
Schizoaffective Disorder
This disorder exhibits psychotic symptoms for a 6 month period while also enduring bi-polar or major depressive disorder must be present through the majority of the schizoaffective disorder. It can be specified as bipolar, depressive or catatonia (DSM-V-TR, 2022).
Treatment remains very difficult for many because of the numerous side effects, lack of family and social support, and the damaging effects of the illness for self care but it can help alleviate symptoms and help some individuals live normal lives.

Medically, since the 1950s, anti-psychotics have proven to be a powerful tool in helping individuals with psychosis and schizophrenia. Also, referred to as neuroleptics, these drugs are dopamine antagonists that reduce the production of dopamine (Barlow, et al., 2022). While helping many individuals who suffer from schizophrenia, the medications can also cause numerous side effects from weight gain to fatigue. Uniquely to schizophrenia, the lowering of dopamine can cause tremor like symptoms similar to Parkinson disease. Ironically, individuals who take medications to increase dopamine for Parkinson disease can experience schizophrenic like hallucinations (Barlow, et. al., 2022).
In addition to anti-psychotics, interventions are key in helping individuals face their delusions and social struggles. Psychotherapy can help individuals understand their way of thinking, as well as provide tools and skills to achieve goals in life while facing the struggles associated with the disorder. In addition, symptom management is essential in identifying warning signs of potential flare ups and when to seek assistance. Social and family assistance is key to helping individuals find their way. Those facing these issues must also always refrain from drugs and alcohol due to their condition of possible psychosis but also due to the nature of the medications they are prescribed (Barlow, et al., 2022). Essentially, it involves not only accepting and discovering that one has this mental disorder but adjusting to a new way of life to manage the symptoms and promote health. Barlow points out that treatment plans should be integrative and include collaborative psychopharmacology, community treatment access, family psychoeducation, supportive employment and illness management skills (2023).
Psychosis while odd and sometimes scary affects many people. Hallucinations, delusions, disorganized speech and negative symptoms are the key groupings of symptoms that manifiest with psychosis. Understanding why it happens and identifying the signs is important in controlling it. It is essential to diagnose and treat before it derails a person’s social, academic, family and professional life. Unfortunately, due to social support, life style change, medicine side effects, and extreme of impairment, many never receive the full help they need. This leads to many be left to fend for themselves as they become more disconnected from reality. Many find themselves homeless, unemployed and in and out of the prison system without proper care.
Please also review AIHCP’s Behavioral Health Certifications for healthcare professionals.
Stress and Trauma Disorders: Access here
Anxiety Disorders: Access here
Mood Disorders: Access here
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorder” DSM-5-TR (5th ed., text revision). American Psychiatric Association Publishing.
Barlow, D.H., Durand, V.M., & Hofmann, S.G. (2023). Psychopathology. An integrative approach to mental disorder (9th ed.). Cengage Learning
McRay, B.W., Yarhouse, M.A., Butman, R.E., & Kiple, C. (2016). Modern psychopathologies: A comprehensive Christian appraisal. (2nd, ed.) IVP Academic
Gregory, S. (2026). “Understanding care and treatments for schizophrenia”. Mayo Clinic. Access here
Schizophrenia (2025). Cleveland Clinic. Access here
Carey, E. (2024). Psychosis. Healthline. Access here
Psychosis: Causes, Symptoms, and Treatment. WebMed. Access here
Those in the fields of stress management, grief counseling, or trauma informed care whether clinical or non-clinical are very familiar with the power of stress, loss and trauma on people. Part of existence is facing struggle and adversity. Stressors and losses, as well as trauma, negatively affect people and force them to adjust, adapt and show resiliency. Obviously, when facing a difficult loss or going through a terrible time, or even witnessing something traumatic, the mind and body reacts. This does not denote pathology but a temporary adjustment to the things, or events that occurred. It would be unnatural not to be sad or unhappy or distressed when bad things occur. It is when these things overcome one’s biology, mind and social support systems that they become unnatural. Instead of finding adjustment, one remains unadjusted through a series of biological or psychological issues that remain persistent. So while not all stress is bad, and while everyone faces loss, and not everyone faces PSTD despite severe trauma, there are cases when pathology and disorder occur that transcends the normal window of reaction in terms of severity and extreme. In these cases, individuals face biological as well as mental problems in adjusting to the issue at hand. This short blog will examine how stressors, loss and trauma can cause disorders as well as the listed disorders in the DSM-V-TR.

Please also review AIHCP’s numerous healthcare certifications for nurses as well as behavioral health professionals, including Stress Management Consulting Certification, Grief Counseling and Trauma Informed Care.
Stress itself is not bad. It is part of life. It pushes one to face adversity and overcome it. Without the push, one would become complacent and not feel the need to improve or provide. Eustress is a term that reflects this reality (Barlow, et al. 2023). Every organism faces stress and stressors. Hans Selye, the Father of Stress Management and the effects of stress on people, pointed out that is sustained stress that gradually breaks down an organism. He listed the first phase of alarm to the stressor, the second phase as resistance to it, and finally the third phase, if resistance failed, which resulted in exhaustion (Barlow, et al. 2023). When an organism reaches a state of exhaustion, it then has biologically, psychologically and socially reached all limits to resist the stressor resulting in disease, breakdown or even death. Chronic stress usually kills over time not immediately but there can be cases when shock and trauma are so great as to cause massive strokes or heart attacks in already vulnerable populations.
Loss is a stressor in itself but loss in itself is not a pathology. Losses in life can range from the smallest things to the most important things. One can lose a job, a relationship, a pet, a parent, or spouse or even a child. These losses, like stressors, vary in degree and intensity based upon numerous subjective elements of the agent or person. For most, losses are tied to love and because of love, there is a sorrow and pain tied to any disconnection. This requires a time to heal and readjust but within normal parameters. It should not impair a person’s ability to live life. When a person is unable to adjust and the severity and length of the sadness overtakes oneself, then a disorder develops.
While everyone experiences stress and loss, traumatic events do not occur to everyone but a high portion of the population does experience them. Like any stressor, trauma while objectively seen as severe can be subjective in how a person responds. The event itself, the experience of the person and its effects play a key role in how a person responds to a particular trauma. When a trauma response activates within a person, which is natural reaction to any extreme event, the response is meant to be temporary for the moment. The survival response in the moment exists in the moment. However, when the survival response becomes a default mode of existence, then disorders such as PTSD emerge.
When stressors or losses or trauma present itself, the body responds. The autonomic nervous systems activates the sympathetic nervous system and one enters into a state of fight, flight, freeze or fawn (Barlow, et al. 2023). The danger part of the brain, the amygdala works closely with the hippocampus and hypothalamus to prepare the body for these modes of survival. The hypothalamic-pituitary adrenocortical axis (HPA) prepares the body for fight or flight or fawn or freeze by inducing states of hyperarousal or hypoarousal to face the threat via injection of cortisol and norepinephrine into the blood stream (Barlow, et al., 2023). This tightens muscles, redirects blood to the core of the body, raises blood pressure, and heightens the person to the moment to react. After the event passes, the body returns to a calmer mode within the parasympathetic system.
When individuals are traumatized, they are unable to turn off this reaction and face a variety of issues. Long term, this can cause numerous health issues, such as hypertension, coronary issues, immune deficiencies, cancer, chronic pain and chronic fatigue (Barlow, et al., 2023).
The DSM-V-TR lists a variety of disorders directly tied to stressors, losses and trauma. They are listed in the DSM-V-TR under the chapter “Trauma-and Stressor-Related Disorders”. The manual states that those who are exposed to traumatic or severe stressful events exhibit in some cases a phenotype which is tied closely to anxiety or fear based issues (2022). In addition, these encounters lead to anhedonic and dysphoric symptoms.
Among the disorders listed, the DSM-V-TR lists Reactive Attachment Disorder (RAD), Disinhibited Social Engagement Disorder, Posttramatic Stress Disorder, Acute Stress Disorder, Adjustment Disorders and Prolonged Grief Disorder (2022).
Attachment Disorders
In regards to attachment disorders, children who experience poor caregiving at a young age develop various reactionary disorders to other caregivers which if left untreated can hinder social relationships in adulthood. This includes RAD which makes it difficult for children to form connections with others (McRay, et al., 2016). Types of attachment behaviors can be avoidant, anxious or disorganized. Each has its own characteristic which hinders a persons ability to foster proper relationships with others (McRay, et al., 2016). AIHCP offers more information about attachment disorders in other blogs that you can review at the bottom.
PTSD
In regards to traumatic response, the DSM-V-TR lists a a long list of criteria and symptoms for PTSD. It states that one must be exposed to actual or threatened death, serious injury or sexual assault in one of the following ways.
In addition, the DSM-V-TR states that the presence of at least one intrusive symptom associated with the event must manifest as
In addition, the person avoids persons, place, stimuli or things that remind them of the event to the point of impairment. They avoid past activities, portray lack of interest and diminished interest with others or the ability to experience positive emotions. The person is also negatively effected in cognitions and moods through inability to remember certain parts of the event, persistent or exaggerated beliefs about oneself or the world or meaning of life due to the event, as well persistent or distorted cognitions about the cause or consequences surrounding the event (APA, DSM-V-TR, 2022). The person will also experience issues associated with their autonomic nervous system. The sympathetic and parasympathetic nervous systems are overworked and experience hypervigilance, exaggerated responses, sleep disturbances, as well as problems with concentration (APA, DSM-V-TR, 2022). PTSD can be specified with either depersonalization, or the separation and detachment from self, or derealization or the feelings that the world around them is unreal. These symptoms must manifest for longer than a month.
Acute Stress Disorder
Acute stress disorder shares many of the similar diagnosis criteria as PTSD, but it is far less severe and lasts from day 3 to 1 month with symptoms diminishing within that time frame (APA, DSM-V-TR, 2022).
Prolonged Grief Disorder
When grief becomes complicated, it can lead to depression, prolong grief disorder or a mixture. The key difference is the locus of the melancholy is due to a targeted and specific loss (APA, DSM-V-TR, 2022). The grief itself is intense and severe and lingers, hampering a person’s ability to function in life. The duration for diagnosis is 12 months after the loss, 6 months for children (APA, DSM-V-TR, 2022). Unlike normal grief, it fails to adjust and is accompanied by intense yearning and longing for the deceased with an abnormal level of preoccupation with the loss. It includes identify disruption, continued shock and disbelief of the loss, intense emotional pain, difficulty with reintegration into life, emotional numbness, a feeling of meaningless and an intense loneliness (APA, DSM-V-TR, 2022). Of course, many of these feelings are felt within the first days, weeks and months of a loss, as well as sometimes on memorial days of the loss. This is why the 12 month deadline is so important before any type of diagnosis.
Adjustment Disorders
Adjustment disorders are tied to life stressors and losses. They illustrate behaviors or emotions that are in response to an identifiable stressor such as a loss, divorce, or loss job. The marked distress is not proportionate to the severity or intensity of the stressor (APA, DSM-V, TR, 2022). It is important to rule out natural loss, prolonged grief, as well as other cultural beliefs that can affect how people react to stress. These adjustment disorders exist within 3 months of the initial stressor
Treatment of anxiety and depression or trauma is best met with psychotherapy. No particular psychotherapy has been proven clinically to be superior or with better results as others but usually a combination of psychodynamic, behavioral and human centered counseling therapeis are key in helping individuals face their issues. Cognitive Behavioral Therapy is very helpful in helping individuals face distorted thinking and form better behaviors. Exposure therapies also exist for cases of trauma to help heal the limbic and sympathetic nervous systems. Included in this is the practice of Eye Movement Desensitization Reprocessing or EMDR. Holistic treatments that focus on meditation, breathwork and hypnosis can help the subconscious heal as well. Medication wise, numerous SSRIs, limited use of Benzodiazepines, and anti-psychotics can be utilized (McRay, et al, 2016).

Helping individuals with stress, anxiety, loss and trauma is part of life. In a world where bad things happen, individuals are forced to face terrible things. Some are minor, while some can overwhelm, and still, some that overwhelm can cause pathological disorders. The diathesis for disorder is based off many subjective issues ranging from biological to psychological to social to cultural and spiritual. In many cases, these life issues can be faced in a non-clinical fashion but when disorders arise, clinical help is required. It is important to remember when working in these fields to remain within the scope of one’s practice.
Please also review AIHCP’s Stress Management, Trauma Informed Care and Grief Counseling Programs.
Attachment Disorders: Access here
Complications in Grieving. Access here
Trauma Informed Care on PTSD/C-PTSD. Access here
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorder” DSM-5-TR (5th ed., text revision). American Psychiatric Association Publishing.
Barlow, D.H., Durand, V.M., & Hofmann, S.G. (2023). Psychopathology. An integrative approach to mental disorder (9th ed.). Cengage Learning
McRay, B.W., Yarhouse, M.A., Butman, R.E., & Kiple, C. (2016). Modern psychopathologies: A comprehensive Christian appraisal. (2nd, ed.) IVP Academic
Acute Stress Disorder. My Cleveland Clinic. Access here
Blain, T. 2025). An Overview of Trauma and Stressor-Related Disorders. Very Well Mind. Access here
Sherrell, Z. (2024). Types of stress disorders. Medical News Today. Access here

Written by Elizabeth Vance
It’s impossible for clinicians to remain effective in their chosen field if they are not continually expanding their understanding of the talking points that matter most within it, and the updated research and methodologies that are regularly published and revised. And that’s no more true than in the case of behavioral health specialists, although the sheer volume of material available for those looking into continuing education (CE) may be an obstacle in its own right, as knowing which route to take when confronted with a multitude of potential CE paths can cause consternation and indecision.
Put simply, it pays to be strategic, as you want the outcomes to be well-suited to your moment-to-moment effectiveness in a role that can be fraught with flashpoints and crises you’re expected to overcome. More than that, CE decisions are as much financial as they are practical, because you want the cost of any course you commit to to be justified, and that involves exploring funding options as much as calculating the effect it will have on your career trajectory and earning potential.
Any clinician who goes ahead with a well-chosen CE strategy should end up with a better-honed set of diagnostic skills, while, in turn, benefiting from better patient outcomes and simultaneously reaping the rewards of a lower-stress workload. With the fears over practitioner liability at fever pitch, it’s reasonable to take this last point as a real motivator to make good choices.
Last but not least, giving a hoot about which CE topics to pick makes sense because of how integrated and overlapping the current medical system has become, with an increased emphasis on practical demonstration of skills and knowledge acquired through CE as opposed to industry bodies and boards accepting passive acquisition. With all that taken into account, now’s the perfect time to dissect and discuss exactly which topics need to be on the watchlist of any behavioral health clinicians, for which purposes we’ve put together an overview of eight core areas that are worthy of focus.
Static risk checklists and binary screening tools have proven fundamentally inadequate because they treat an evolving psychological crisis like a rigid bureaucratic inventory. Modern clinical competency demands an immediate transition from rudimentary suicide risk screening to advanced, collaborative risk formulation models that account for fluctuating internal and external variables. Clinicians must possess the training required to systematically parse chronic, static baseline vulnerabilities from immediate, acute, near-term destabilizers to construct dynamic, highly personalized safety plans.
This advanced approach directly aligns with the highly structured Assessing and Managing Suicide Risk frameworks utilized by major national health systems to drastically minimize provider legal liability while substantially improving acute patient outcomes. Rather than relying on outdated “contracts for safety,” which offer no legal or clinical protection, advanced coursework trains clinicians to co-create proactive crisis response plans with patients. These contemporary frameworks emphasize the meticulous documentation of clinical decision-making, ensuring that a practitioner can clearly demonstrate an objective, defensible standard of care in high-stakes clinical environments.
Furthermore, advanced suicide risk formulation requires a deep understanding of the intersection between acute psychological pain and cognitive constriction, a state where a patient’s problem-solving capacity drops to near zero. Continuing education in this domain instructs the healthcare professional on how to conduct nuance-driven phenomenological interviews that uncover implicit suicidal intent that standard check-box metrics routinely miss. By mastering these sophisticated interviewing techniques and formalizing objective risk formulation documentation, behavioral health professionals effectively bridge the gap between abstract ethical mandates and real-world clinical survival.
An exceptional, highly sophisticated clinical intervention completely loses its real-world efficacy the moment a vulnerable patient steps out of a clinical office into a severely fractured, unstable home environment. True, long-term continuity of care relies heavily on a behavioral health clinician’s systemic ability to analyze and navigate complex social determinants of health, including stable housing, nutritional security, legal protections, and localized support networks. Continuing education must empower healthcare professionals to look past the individual psyche and master macro-level community resource mapping.
Clinicians frequently need to coordinate with dedicated local medical networks to ensure their patients receive comprehensive, localized support during the critical recovery and reintegration phases. For example, linking individuals to established, highly structured mental health treatment programs in Indianapolis, IN provides a vital, real-world bridge between acute clinical stabilization and sustainable, long-term community reintegration. Mastering this level of resource navigation requires an advanced understanding of healthcare bureaucracy, inter-agency information-sharing regulations, and multi-disciplinary care coordination strategies.
When a behavioral health professional is fully capable of addressing systemic barriers to care, they dramatically reduce patient readmission rates and prevent outpatient treatment drop-outs. Advanced training in resource navigation teaches clinicians how to conduct comprehensive social needs assessments and to build formal, collaborative partnerships with local social service agencies, medical clinics, and vocational rehabilitation centers. This macro-level competence transforms the clinician from an isolated counselor into a powerful, highly integrated navigator within the broader modern healthcare ecosystem.
Trauma-informed care has unfortunately been diluted into a generic industry catchphrase focused on basic empathy, yet true clinical efficacy requires an intricate, operational understanding of neurobiology. Experienced clinicians understand that early developmental trauma and prolonged chronic stress systematically alter the structure and function of the human nervous system, directly impacting adult treatment adherence and physical health outcomes. Continuing education in this highly specialized space must move well beyond basic talk therapy modalities and instead focus on specific, evidence-based somatic and grounding interventions.
Advanced coursework provides practitioners with the explicit technical skills needed to recognize and regulate autonomic nervous system dysregulation, including severe hyper-arousal and dissociative hypo-arousal states. Training programs must detail exactly how to structure clinical interviews to prevent secondary traumatization, protect the therapeutic alliance, and safely manage intense patient disclosures without causing clinical regression. Understanding the exact role of the amygdala, prefrontal cortex, and vagus nerve during trauma processing allows clinicians to apply interventions that are precisely timed to the patient’s window of tolerance.
By gaining deep competency in these physiological interventions, behavioral health professionals transition from simply discussing trauma to actively facilitating structural neurological recovery. This level of sophistication is mandatory for clinicians operating in intensive outpatient programs, acute psychiatric care facilities, and specialized private practices.
The historical, institutional barrier between mental health treatment programs and specialized substance use interventions has completely collapsed across modern clinical environments. Attempting to treat a severe substance use disorder without simultaneously addressing the underlying psychological drivers, or vice versa, routinely traps the patient in a costly, demoralizing cycle of rapid relapse and re-hospitalization. Contemporary behavioral health education must abandon the outdated model of parallel or sequential treatment and fully embrace sophisticated, integrated co-occurring disorder protocols.
Coursework must focus heavily on simultaneous care models in which a single clinical team addresses both diagnostic profiles within a unified treatment plan. Clinicians are required to master the nuances of concurrent psychopharmacology tracking, identifying how specific illicit substances interact with prescribed psychiatric medications, and adapting counseling strategies accordingly. This high-level training allows professionals to accurately differentiate between substance-induced psychiatric symptoms and independent, primary Axis I mental health conditions, a distinction that fundamentally alters long-term prognosis.
When clinicians operate with an integrated dual-diagnosis framework, they can effectively decode the functional utility of a patient’s substance use, treating it as a maladaptive, highly organized attempt at self-medication. Continuing education in this domain directly empowers the healthcare professional to design sophisticated behavioral interventions that replace the substance’s functional role with adaptive psychological coping mechanisms. This integrated approach dramatically reduces treatment dropout rates and ensures alignment with modern managed care organization utilization review criteria.
The rapid, unmanaged evolution of digital health platforms and generative artificial intelligence has significantly outpaced legacy state licensing board regulations and ethical codes. Simply knowing how to log in to a HIPAA-compliant video platform is no longer sufficient to ensure clinical, ethical, and legal compliance in telehealth delivery. Contemporary continuing education must comprehensively address the legal nuances of cross-jurisdictional practice boundaries, emergency crisis management across state lines, and the security liabilities of emerging AI-driven documentation systems.
Practitioners require explicit, advanced instruction on digital privacy laws, encryption protocols, and the specific administrative safeguards needed to protect sensitive protected health information from sophisticated cyber threats. Furthermore, as behavioral health platforms increasingly integrate artificial intelligence for preliminary diagnostic screening and progress note generation, clinicians must understand the profound ethical risks regarding data ownership and algorithmic bias. Advanced training teaches the clinician how to maintain complete human oversight, ensuring that AI tools are utilized strictly as administrative supplements rather than replacements for independent clinical judgment.
Managing a remote therapeutic relationship also requires a highly specialized set of clinical skills to compensate for the loss of physical, in-person environmental cues. Advanced telehealth coursework trains behavioral health professionals to systematically assess a patient’s suitability for remote care, establish rigid environmental safety protocols, and manage acute technical disruptions during high-anxiety moments. By securing this technical and legal mastery, healthcare providers protect their clinical licenses while maximizing the geographic reach and accessibility of their specialized services.
Legacy cultural competence courses frequently relied on overgeneralized demographic summaries and rigid cultural profiles that inadvertently reinforced clinical stereotypes rather than dismantling them. Modern healthcare delivery demands a definitive behavioral shift toward continuous, deeply self-reflective cultural-humility frameworks that prioritize the unique intersectional identity of each patient. Advanced continuing education in this domain equips practitioners with the rigorous tools needed to identify and neutralize implicit clinical biases that undermine diagnostic accuracy and treatment planning.
Practitioners require specialized education on the complex social determinants of health, systemic medical disparities, and the distinct historical barriers to care that marginalized communities continuously encounter. This sophisticated approach goes far beyond basic clinical empathy, instructing the behavioral health provider on how to modify evidence-based protocols to align with diverse worldviews, linguistic nuances, and community structures. By developing this advanced competency, clinicians significantly strengthen the therapeutic alliance, which peer-reviewed metadata consistently identifies as the single greatest predictor of positive therapeutic outcomes across all demographic groups.
Understanding the unique stressors associated with minority status, systemic economic disenfranchisement, and cultural institutional trauma allows clinicians to accurately contextualize symptomatic presentations. Advanced training ensures that healthcare professionals do not pathologize adaptive survival behaviors or cultural expressions, leading to far more accurate diagnostic formulations. Ultimately, integrating radical cultural humility into the diagnostic process elevates the ethical standard of the entire behavioral health industry, creating a highly equitable healthcare environment.
Major commercial insurance payers and federal Medicaid frameworks are rapidly shifting their reimbursement structures to reward concrete, empirical clinical data rather than subjective provider progress notes. Providers who fail to demonstrate verifiable patient progress through the systematic utilization of standardized psychometric tracking tools face increasingly severe utilization reviews, retroactive billing audits, and outright payment denials. Measurement-based care is no longer an optional academic exercise; it is an administrative and clinical mandate for the modern behavioral health professional.
Advanced continuing education programs must train clinicians to seamlessly integrate standardized screening instruments, such as the PHQ-9, GAD-7, and PCL-5, into their day-to-day clinical workflows. Rather than treating these assessments as cold, intrusive administrative hurdles, advanced training teaches the clinician how to share this empirical data transparently with the patient to enhance engagement and collaborative goal-setting. Utilizing these data-driven insights allows clinical teams to rapidly refine treatment plans in real time when a patient’s progress plateaus, safeguarding billing compliance while significantly improving clinical outcomes.
Furthermore, mastering clinical outcome analytics enables behavioral health directors and private practitioners to aggregate data across their entire clinic population to identify systemic clinical trends. This macro-level data utilization is highly valuable when negotiating reimbursement rates with major insurance panels or applying for federal health service grants. Gaining absolute competency in measurement-based care effectively bridges the traditional gap between empirical clinical science and the pragmatic, day-to-day business of healthcare delivery.
Relying exclusively on local emergency services or immediate psychiatric inpatient hospitalization is an unsustainable, clinically disruptive approach to managing behavioral health crises in outpatient environments. Clinicians must possess an advanced toolkit of verbal and nonverbal de-escalation interventions designed to safely defuse high-tension, high-acuity scenarios as they materialize. Advanced continuing education provides highly specialized techniques for managing acute behavioral agitation, intense panic states, and oppositional, combative behaviors within a standard office or community setting.
This advanced training instructs the healthcare professional on the subtle nuances of proxemics, kinesics, and paralanguage, detailing how a clinician’s physical positioning, body language, and vocal tone can either rapidly diffuse or inadvertently exacerbate a volatile situation. Practitioners learn to systematically identify the early physiological signs of impending behavioral escalation, allowing them to intervene proactively before a patient completely loses cognitive control. Mastering these advanced defusing skills directly protects practitioner and staff safety while simultaneously minimizing unnecessary, highly restrictive institutional interventions that can severely traumatize the patient.
Additionally, comprehensive de-escalation training outlines the precise legal and ethical boundaries of crisis intervention, ensuring that any physical or environmental management fully complies with state regulations. Clinicians learn to execute meticulous post-crisis documentation that outlines the specific antecedents, the exact verbal interventions attempted, and the collaborative resolution reached. This level of clinical precision safeguards the practice from regulatory scrutiny while preserving the therapeutic relationship after a high-stress clinical rupture.
Prioritizing highly structured, sophisticated professional development ensures that a behavioral health practice remains both ethically unassailable and clinically potent within a hyper-regulated healthcare industry. Reviewing advanced internal clinical training indices and seeking out rigorous, peer-reviewed continuing education opportunities allows practitioners to elevate their day-to-day therapeutic interventions from basic supportive therapy to highly advanced clinical science. Commitment to this ongoing professional evolution is the definitive hallmark of a dedicated healthcare professional focused on delivering true, measurable patient recovery.
Dr. Elizabeth Vance, LCSW, PhD, is a senior clinical consultant and behavioral health strategist specializing in high-acuity crisis formulation and clinical operations management. With over two decades of experience directing multi-disciplinary medical and psychiatric teams in intensive outpatient environments, Dr. Vance designs advanced continuing education curricula for licensed health professionals nationwide. Her peer-reviewed research focuses heavily on the neurobiology of trauma and the systematic integration of measurement-based care frameworks into private and institutional healthcare practices.
Please also review AIHCP’s Certification program and our CE courses as well, to see if they meet your academic and professional goals. These programs are online and independent study and open to qualified professionals seeking a four year certification
Anxiety is one of the most common mental and emotional ailments clients face. Ironically, anxiety is natural part of life. It is intimately tied to the nervous system to help push individuals. Just like stress, it can help serve individuals to meet deadlines, face problems, and persevere under pressure. To remove all stress and stressors would be a bad thing in life, as well as to remove all future angst about future issues. Anxiety itself is ontological and part of one’s being. It is part of being alive (McRay, 2016).

The DSM-V-TR defines anxiety as “anticipation of future threat (2022)”. However, when anxiety is not proportionate with the actual threat, then it becomes a malignant worry. It creates a negative mood, but the mood becomes excessive and creates a variety of somatic physiological symptoms and tensions when it becomes a disorder (Barlow, et al., 2023). So, if a student has anxiety the night before an exam, this is not reflective of an anxiety disorder, but a true reflection of potential worry of not passing the exam, however, if a student exhibits consistent worry about not being good enough to succeed in life and this filters into almost every venue of life, then one can see where anxiety can unravel into pathology.
Please also review AIHCP’s Healthcare Certification programs in mental health.
How one reacts and handles stressors and future problems is key to living a successful life. It is not about not feeling these interior movements, but being able to cope with them and maintain them within normal levels. There are biological, psychological and social conditions that need to be considered to explain why some individuals are more prone to anxiety disorders than others. Biologically, individuals with anxiety disorders have lower levels of gamma-aminobutryic acid (GABA) which helps keep the neurons from firing and hence keeps individuals calmer (Barlow, et al., 2023). In addition, some individuals have issues within the limbic system and its association with fight of flight. An overstressed autonomic nervous system can keep a person’s sympathetic branch more alert and on fire due to past trauma. While PTSD is now considered a trauma disorder, anxiety is still closely tied to PTSD, and individuals suffering from a variety of anxiety disorders also experience overactive sympathetic branches (Barlow, et al., 2023).
Psychologically, there are different interpretations for why anxiety exists in some and not others. Psychoanalytic schools of Freud see anxiety a severe mechanical break down of systems. Freud considered anxiety to be an internal warning sign of the ego regarding subconscious conflicts or forbidden impulses. Behaviorists considered anxiety to be due to learned behavior regarding modeling from others or cognitively through uncorrelated ideas about the self and one’s surroundings (McRay, 2016). Parents who teach their child control and predictability also help create a healthy mindset for healthier thoughts about life, coping and resiliency (Barlow, et al., 2023). In addition, parents who are overbearing and controlling, impede the child’s ability to become resilient and also incur interior fears about life that can later manifest as anxiety.
Social factors also play a key role in one’s dance with anxiety. Past traumatic events can weaken the autonomic nervous system. In addition, numerous losses, as well as interpersonal distresses ranging from divorce to loss of a family member can lower one’s ability to resist future anxiety disorders. These disorders then can effect other aspects of social functioning (Barlow, et al., 2022).
Spiritually, one’s faith can also play as a key anchor against anxiety. In fact, any world view or existential meaning in life can help one find security in times of angst. Existentialist philosophy teaches that the world is filled with trouble, loss and anxiety but it how one faces it that determines one’s control of life direction. Instead of avoidance, hiding, or fear, world views can help individuals find courage, fortitude and faith in their direction.
An integrated model for anxiety vulnerability best illustrates why some succumb to anxiety disorders and others do not. One must look a diathesis models that look at genetic vulnerabilities, life stressors, and mental and cognitive world views that all come together to overwhelm an individual. Biological vulnerabilities include inherited traits. Generalized psychological vulnerabilities include world views, such as believing the world is a dangerous and unsafe place. Finally, specific psychological vulnerabilities are what one learns from individual experience or what is taught in childhood (Barlow, et al., 2022). When an event occurs that challenges everything, some individuals may be weakened enough to enter into a disproportionate response of anxiety.

The DSM-V-TR lists 7 anxiety disorders. Again, it is important to notate, OCD and PSTD are no longer listed with core anxiety disorders albeit they exhibit anxious symptoms and are closely related. In addition, hoarding and various picking at self disorders are tied with OCD. The manual follows life span development as its means of listing order for anxiety, as well as all disorders. It lists Separation Anxiety, Selective Mutism, Phobia, Social Anxiety Disorder, Panic Disorder, Agoraphobia, General Anxiety, and Substance/Meditation-Induced Anxiety Disorder (DSM-V-TR, 2022).
In this short blog, we will look at General Anxiety Disorder (GAD), phobias, Social Anxiety Disorder (SAD), Panic Disorders with Agoraphobia and Separation Anxiety. Please also review AIHCP’s Stress Management Program.
GAD
General Anxiety Disorder involves unsubstantiated worry over numerous dimensions of life and is not just tied to one thing, such as an attachment to one person, or how one is viewed in public. The disturbances are excessive in nature and occurring for more days than not over a period of 6 months. The individual is unable to stop or control worrying. The symptoms are tied to restlessness or being on edge, fatigue, difficulty concentrating, irritability, muscle tension and sleep disturbance. The DSM-V-TR states that only 3 or more of these symptoms are required. Key to the diagnosis is that the anxiety causes extreme impairment in social, occupational, or other important areas of functioning (DSM-V-TR, 2022). GAD is also associated with increase suicidal thoughts and behaviors. It also can have a comorbidity with depression disorders. Anxiety is usually tied at a higher percentage to women but also occurs in men.
Selective Phobias
Phobias are unrealistic reactions to things that cause heightened anxiety even without the object or thing or place present. Natural to survival and the autonomic nervous system is the reaction to fear through the sympathetic branch and its fight or flight responses. Hence fear is a negative effect within the sympathetic nervous system that alarms the body to present danger (Barlow, et al., 2023). It is important to note that many fears that become phobias are tied to natural biological and evolutional reactions. Avoiding the dark, or being careful in high places, or be cautious around potential poisonous creatures as snakes or spiders are good things but phobias hijack the sympathetic nervous system and cause disproportionate anxiety to these things even when they are not present. Phobias are coded in the DSM-V-TR according to animals such as snakes or spiders, natural environment such as heights, water or storms, blood injection-injury such bodily fluids, needles, or injections, or situational such as airplanes, elevators or enclosed places (2022).
Diagnosis involves a heightened and fearful anxiety regarding any of the listed phobias. The situation or thing must always provoke immediate anxiety or fear. These things or places are actively avoided or endured with intense fear. The fear or anxiety is out of proportion with the reality of danger. The fear or anxiety is persistent for 6 months are more. The fear or anxiety causes social impairment in social, occupational or other areas of functioning and these symptoms are not explained through other mental or substance issues (DSM-V-TR, 2022).
SAD
Social anxiety disorder is anxiety that is disproportionate based on social implications of performance, speaking, or being in social settings. Ironically, for some performers, regular social settings may not cause anxiety but for others everyday interaction in social settings, even if they are not speaking or performing can cause anxiety. Hence these individuals become extremely nervous even in school, or parties, or other events. It revolves around perceptions of how they perceive they are seen, or viewed by others. A microscopic lens is placed over every action or word they say. This may be due to fear of rejection, embarrassment or ridicule. While again, it is natural sometimes to feel some anxiety within social norms in everyday life or if performing the next day, the anxiety associated with SAD impairs functioning. It overtakes the person and causes intense somatic symptoms even upon the thought of social activity. In addition, panic attacks can associate with SAD prior to an event or during a social setting. Many sometimes will completely avoid functions, or mask it with substance abuse issues. Social anxiety disorders are more highly diagnosed with women and also children entered into their teen age years but can happen to both men and women.
Sometimes closely tied to SAD is body image. Since SAD focuses on anxiety surrounding on perceptions of others, Body Dysmorphic Disorder can play a big role especially in teens. BDD focuses on minute or even non-existent perceived flaws in the body. This subjective issue becomes a obsessive pursuit through various compulsions to alter or make better these small blemishes. For some, this disorder is then tied to SAD.
The DSM-V-TR utilizes the following diagnosis criteria. It lists marked fear or anxiety regarding one or more social interactions that expose an individual to possible scrutiny that involves conversations, social events, dates, meeting unfamiliar people, as well being observed by others. The manual notes that individuals feel they will be negatively evaluated, humiliated, or embarrassed or rejected. The social settings must always provoke fear or anxiety. In addition, the individual will look to avoid these settings and the fear and anxiety is out of proportion with the actual sociocultural context. The fear or anxiety must present itself for 6 months or more and causes intense impairment. These conditions are not attributed to other mental disorders or substances (2022).
Panic Disorders and Agoraphobia
Panic disorders are continual and persistent panic attacks. Arogaphobia is fear of public places with crowds due to the fear of possible panic attacks. Both are separate disorders but are tied closely together due to the nature of panic attacks. Panic disorder according to the DSM-V-TR is a recurrent phenomenon where an abrupt level of anxiety manifests within minutes. It can be expected or triggered or even unexpected in some cases. The attacks can occur one per week for months, or less frequent attacks separated by weeks or months. Not all panic attacks are tied to Panic Disorder since some panic attacks are tied to Social Anxiety Disorder. Panic Disorder and panic attacks cause somatic physiological symptoms that include palpitations, sweating, trembling, shortness of breath, feelings of choking, chest pain, nausea, dizziness, chills or heat sensations, paresthesias, derealization, and fear of loss of control or dying (2022). The DSM-V-TR also states that anxiety and fear over future panic attacks are followed within the month, especially in regards to the symptoms, as well as maladaptive measures to avoid future panic attacks (2022). Of course, these disturbances are not due to any other diagnosed mental issue or substance or medication.
Those who suffer with Agoraphobia fear public situations where possible panic attacks could occur and the embarrassment or issues that may occur if in a public area because of it. The DSM-V-TR lists public transportation, open public spaces like super markets or parking lots, enclosed places like theatres, large crowds or standing in line, or being alone outside of the home. The person faces extreme anxiety over these thoughts and will actively look to avoid these places to the point of impairing one’s social, professional and academic life. The fear is disproportionate, persistent and lasts for over 6 months and is not caused due to other diagnosed mental illness, substance or medication (2022).
Separation Anxiety
Separation anxiety deals with intense disproportionate fear and dread of being separated from a caregiver, loved one, or a child. It is more common in children but can also manifest in adults with children. This should not be misinterpreted for natural anxiety after a traumatic event or even a new parent, but is a persistent and disproportionate reaction that involves fear and dread of losing a loved on or something bad happening to oneself when the loved one is not present. Traumatic events, unhealthy attachments as a child, or overbearing parenting can lead to potential development of Separation Anxiety Disorder.
The DSM-V-TR states criteria for diagnosis states that excessive fear or anxiety regarding anxiety must manifest in three or more examples. Recurrent or inappropriate fear when anticipating or experiencing separation. Persistent worry about losing a major attachment figure to illness, injury, disaster or death. Worry of kidnapping, accidents, illness, or unfounded events. Refusal to go other places for fear of separation with figure. Persistent fear about being alone with the other figure. Trouble sleeping without or being away from home without the other figure. Repeated nightmares involving the scheme of separation with the figure and somatic physiological ailments such as headaches, stomach aches, vomiting and nausea stemming from the anxiety (2022). These issues must persist for 6 months in adults and 4 weeks in children and cause impairment in all social spheres of life. Again, it cannot be attributed to other mental illness, substance or medication.
Treatment

In all of these cases of anxiety, suicidal ideation can be a symptom to closely monitor. Obviously, some individuals will exhibit mild, moderate or severe and need treatments based on their individual needs. In addition, it is important during treatment to be aware of any comorbidities such as depression that may exist with presenting problem or diagnosis. It is also important to be mindful of cultural aspects that can normalize certain actions that may seem abnormal to other cultures. Finally, it is important to be delicate in diagnosis to prevent labeling and other mental health stigma (DSM-V-TR, 2022).
In clinical settings, Cognitive Behavioral Therapies (CBT) are the most utilized behavioral therapy to help the person reframe and rethink their anxieties. Some individuals with Anxiety Disorders have a recognition of of illogical thinking despite the feelings and can rationalize while others have differing levels of lack of logical thinking and are completely controlled by these thoughts. For instance, an adult with Separation Anxiety Disorder may acknowledge the improbability of bad things occurring to loved a one but still feel the anxiety while others may be completely under the delusion that something will happen. This happens also in cases of hoarding and OCD. CBT can help individuals better rationally reframe reality from fantasy and help individuals rethink what they are experiencing. For instance, someone who is facing Social Anxiety Disorder, may be able to reframe negative images and perceptions of what others are thinking into positive and more likely things, or even recognize that their perception of being the center of attention is not a reality. In regards to phobia, exposure therapies are a key way to help individuals face exaggerated anxiety. Many behaviorists believe that pathology is tied to operant and classical conditioning during childhood. How someone was raised or how their behavior was influenced plays key roles to phobias and anxiety. With phobias, new learned experiences can help reshape the neuroplasticity of the brain and how it perceives threats. Exposure therapies gradually create new experiences (Barlow, et al., 2022).
In addition to CBT and other cognitive behaviors, pharmacological treatments can help alleviate anxiety. Benzodiazaphines can help GABA levels become more stable and calm the person (McRay, 2016). Xanax, as well as Ativan can help alleviate the intense lack of calm and anxiousness and help the person find peace but it is important to note that long term use of these drugs exceeding 2 weeks or a month can lead to addiction. Hence these drugs are more for acute purposes instead of long term treatment. Many issues associated with anxiety is also tied with serotonin levels. SRRI can play a role in helping regulate mood. Paxil is a common drug used to help individuals with anxiety that can be used long term and help regulate mood (Barlow, et al., 2023).
Other holistic and natural remedies can also be utilized. Supplements for GABA under the care of a healthcare professional can be utilized as well as calming techniques, meditation, and prayer. In addition, hypnosis and EFT can also play key roles in helping manage anxiety. Please review AIHCP’s EFT Practitioner Program
From a Pastoral approach, pastoral care givers should be ready to refer clients to clinical professionals but they can also aid with coping skills, reframing, and helping individuals find meaning. For Christians, biblical approaches that tie the person to the life of Christ and how biblical characters faced anxiety can be modeling examples. In addition, how does one’s faith approach anxiety and worry? Analyzing faith and teachings can help build resiliency within the person. Spirituality is many times forgotten or swept under the rug, but spirituality plays a key role in how one thinks and feels in life. It is hence important to include pastoral approaches that address existential and spiritual explanations for anxiety in life (McRay, 2016).

Anxiety is natural but also the most common mental malady. Diagnosis is not a simple process but a complex one. While all these disorders differ in some degree, the primary culprit is a disproportionate anxiety response. Causes can range from biological, psychological, social and spiritual in nature. Helping others understand and sometimes helping them at a medical level is key to helping control and maintain anxiety.
Please also review AIHCP’s Stress Management Consulting Program as well as AIHCP’s multiple healthcare certifications in grief, crisis, anger, meditation, trauma informed care and spiritual counseling.
Stress Management and Anxiety Disorders, Click here
EFT and Anxiety. Access here
Anxiety Disorders. Mayo Clinic. Access here
Anxiety Disorders. Cleveland Clinic. Access here
Guy, Evans, O. (2025). “7 Types of Anxiety Disorders: Signs, Causes, & Management”. Simply Psychology. Access here
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorder” DSM-5-TR (5th ed., text revision). American Psychiatric Association Publishing.
Barlow, D.H., Durand, V.M., & Hofmann, S.G. (2023). Psychopathology. An integrative approach to mental disorder (9th ed.). Cengage Learning
McRay, B.W., Yarhouse, M.A., Butman, R.E., & Kiple, C. (2016). Modern psychopathologies: A comprehensive Christian appraisal. (2nd, ed.) IVP Academic