Many times in counseling when discussing trauma, emotions can emerge tied to the unresolved trauma that can de-regulate a client/victim/survivor. Discussing issues of abuse, or loss, or traumatic memories whether current or in the past can cause individuals suffering from unresolved trauma to dissociate from the present, flashback to the past, or enter into states of emotional dysregulation. Licensed counselors who specialize in trauma care and crisis intervention have strong understandings to utilize techniques to help ground and contain negative emotions associated with trauma. Unlicensed mental health professionals in crisis response or even pastoral care may sometimes come across individuals who also need these same techniques due to acute crisis or trauma. It is hence important to understand how to help individuals suffering from PTSD, acute trauma, or unresolved trauma with the appropriate techniques to help victims or survivors find stabilization. This article will focus more on in session counseling and long term trauma care than immediate psychological first aid which is addressed in other blogs. Primarily, we will discuss the therapeutic relationship’s window of tolerance with a victim/survivor, how to expand this window, and review various techniques found in grounding and containment to help others find calm and peace.

Please also review AIHCP’s Trauma Informed Care Certification, as well as its Crisis Intervention program and also all of AIHCP’s Healthcare Certifications.
Window of Tolerance
In counseling, individuals can experience emotional dysregulation due to unresolved past trauma. Simple triggers of retelling the story, to similar images in a room, or a familiar scent can reset a person and dissociate, flashback, or cause intense states of hyperarousal or hypoarousal. Compton explains that individuals can experience two types of dysregulation. In hyperarousal, the person becomes angry, anxious, hypervigilant, or impulsive (2024, p. 208). Compton points out that with hypoarousal the opposite occurs when the person experiences withdraw, numbness and lack of emotion even in some cases to a state of dissociation (2024. p. 209). In the fight or flight response, counselors will see anger and anxiety, but during the freeze response, counselors will see the shutdown. These are natural ways the body and brain responds to past trauma. The key is how easily can one’s system return to a state or emotional regulation when dealing with these triggers or reminders that cause emotions to emerge. Individuals in trauma can be stuck in a variety of phases, some may exist in a state where they feel no safety anywhere, others may exist in a state where safety may not be an issue but trust is totally lacking. It is the goal of the counselor through the therapeutic relationship to help victims again find phases of regained power, regained self esteem and eventually the phase where they can again reintegrate with society and form healthy relationships. It is within the Window of Tolerance of a person’s emotional state where this healing can occur.
The Window of Tolerance is term phrased by Ogden, Minton and Pain that refers to the optimal window of time between hyper and hypoarousal states in which a person can experience balance (Compton, 2024, p. 209). Within this period of time, therapeutic counseling can occur where the trauma can be discussed and better ways to cope can learned by the client. During this time as well, the reasoning part of the brain as opposed to the emotional part has more awareness to communicate, reason, learn and grow (Compton, 2024, p. 209). Counselors can help clients learn how to operate and heal within the window but also learn ways to expand this window in real world settings through a variety of skills. Counselors can help clients co-regulate their emotions within the window and expand it through supplying empathy, support, a safe and secure environment and also preventing re-trauma by limiting or eliminating potential triggers.
Counselors during this time through the therapeutic relationship can help with focusing on the needs of the client and being aware of discomfort or physical manifestations associated with mental discomfort. Compton points out that the term “interoception” best describes the ability of a counselor to have this type of awareness of what is happening inside someone based on what the body is displaying or doing in the moment (2024, p. 196). this is why watching for non-verbal cues is key in counseling during the selective attention skill of focusing. During this important window, counselors should engage their clients. By focusing, reflecting and providing context, counselors can help survivors understand their trauma better (2024, p. 197). In addition to engaging, counselors need to help clients process emotion and then help them reflect on it. The biggest part of processing is not only discussing it, understanding it, and reframing it but to also learn how to manage it.
Tracking and Identifying Emotional States
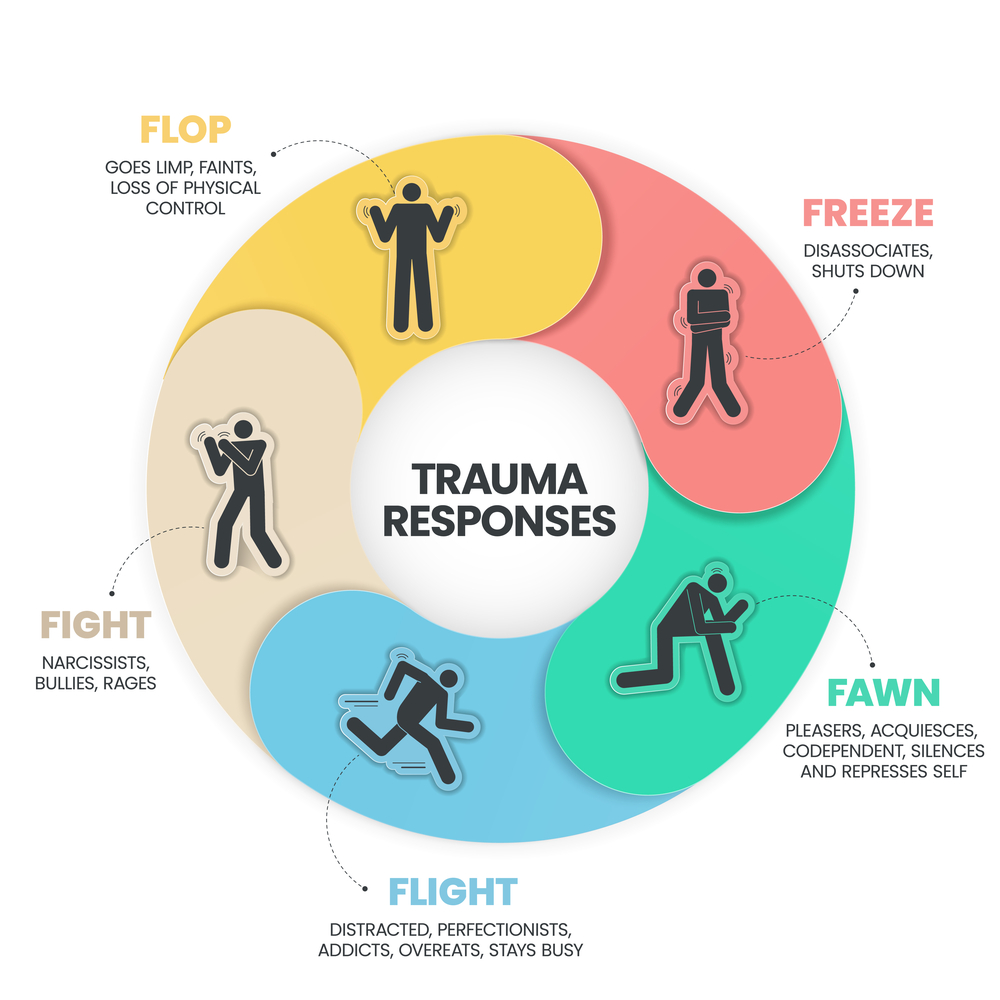
Within trauma counseling, it is important to utilize the window of tolerance but it is also equally important to track the client’s body and behavior for signs of either hyperarousal or hypoarousal. It is also important to track oneself, since sometimes the stories and events relayed can even shock a counselor and cause deregulation within. It is important to note that most individuals exist within a normal operating existence of balance when viewing safety and conditions. The securing of safe environments and the scanning by the brain to ensure safety within a environment is referred to as neuroception. A person in a calm and secure state is not activating the sympathetic nervous system but is existing in normal state where the cognitive functions of the brain are operating. When the sympathetic nervous system strikes it can close down cognitive functioning and increase emotional responses. Fight, flight or freeze, or even fawn can emerge as reactions to this. Interesting enough in cases of hypoarousal, the parasympathetic system, the calming aspect of our nervous system, can deactivate an individual due to the intensity of the trauma or recalling the trauma. When working with survivors or victims, merely recalling traumatic events can cause a hyper or hypoarousal response. This can affect healing and reduce the window time tolerance to discuss the trauma with the cognitive functions operating.
Tracking emotions and signs is hence an important skill for a counselor in any session but even more so when helping individuals in intense grief, loss, crisis or intense trauma. In states of hyperarousal a person will display various physical and also behavioral symptoms. In essence the person cannot calm down. Clients in hyperarousal can display anxiety, irritability, panic or rage. They may have racing thoughts, or an inability to concentrate and may display signs of hypervigilance during the session. Physically they have increased heartrate, muscle tension, clenched jaw, closed fists, display sweating or have a racing heart rate. Behaviorally, they can display an overall restlessness which may be affecting their sleep and impulse control. They may fidget and move and express emotions easily during the session. This can lead outside the counseling room to regular life in feelings of being on edge, easily irritated, over-thinking social interactions, and feeling uneasy in social settings (Mindset Explained, 2025).
When tracking, a counselor also needs to track possible signs of hypoarousal. Hypoarousal can be induced by either the sympathetic or parasympathetic. It is usually tied to parasympathetic functions that relax the body but in these cases it shuts the body down as a self defense mechanism to the trauma or even thought of the past event. A person experiencing hypoarousal will display detachment, numbness and seem withdrawn and lacking motivation. Cognitively, they may be slow to speak and appear confused and lacking details about events. Physically they will seem lethargic and have a slower heart rate, display fatigue, or over relaxed muscle state. During a session, they may zone out or seem distracted. Behaviorally this can lead to intense isolation outside the counseling room. Many may have a hard time getting out of bed, or detach from loved ones, feel powerless and lose interest in things they like to do (Mindset Explained, 2025).
In both cases, counselors need to be aware of these signs but also know when to utilize activation strategies for hypoarousal or settling techniques for hyperarousal. In these cases, settling or activating becomes the choice a counselor needs to make. In states of hypoarousal activities that help the person activate the nervous system include helping the client begin to move, via stretching, or walking around can be a first good start. Other ways to activate include grounding techniques that are tied to touch and sense, such a the feeling of a cold object or ice cube, or the splash of water on the face. Other forms of breathwork, as well as cognitive activation through counting or labeling things in the room can also aid the client. Sometimes music can be helpful, or even the scent of a candle (Mindset Explained, 2025).
With hyperarousal, the concern is to settle, not activate. Hence, breathing exercises, ground techniques such as holding something, or touching something, as well as sensory and cognitive ways to help the person remain in the present. Progressive muscle relation techniques as well as guided meditation and visualization can help a person induce the parasympathetic system as well. We will discuss more types of ground and containment strategies later in this article. What is optimal is a stable state of being. Stable and emotionally regulated states allow the window of tolerance to be utilized in therapeutic sessions. Healthy states permit better focus, cognitive functions, stronger relationships, better sleep and better energy levels to cope with stressors and potential triggers (Mindset Explained, 2025).
One thing to consider and be aware of is that while helping others, counselors can also enter into various states of hyperarousal or hypoarousal. The term reciprocal defense mobilization is the mirroring of emotional states. While ideally the counselor is the co-regulator in a session providing energy, trust and security to the person, sometimes horrible stories or emotional breakdowns can affect the counselor. In fact, past trauma of the counselor can also be triggered in counseling. This type of vicarious trauma can have acute affects on the session but also long term affects and burnout for the counselor. If a counselor is affected via hyper or hypoarousal, the ability to listen, exercise empathy, or help the person heal can be at risk. Hence counselors may sometimes need to activate or settle themselves. It is harder though for a counselor to express these feelings or exhibit certain strategies while counseling and because of this counselors need to be able to subtly activate or settle themselves. In cases of hypoarousal, a counselor may notice one’s own signs of shutting down and look to activate by clenching one’s fist or hand or shifting or tapping one’s foot. A counselor can also discuss both parties standing up and stretching as a ploy to not only help the client but oneself. A break or a pause can be helpful for both client and counselor in these cases. During hyperarousal, a counselor can label, or count, or focus on one’s own breathing.
One should consider basic strategies to manage both hyperarousal and hypoarousal in daily life. In regards to hypo, utilize frequent exercise if possible, alone, if public gyms are unsettling. Utilize breathing and mindfulness, and create and stick to routines that give a sense of accomplishment and work on connecting with others, especially those who are closest. Even if a short phone call or text! For hyperarousal, one will utilize more grounding techniques in daily life which will be discussed below and also employ relaxation and meditation, as well as with creating a calmer environment with music, or scented candles (Echowave, 2025).
Grounding and Containment
A person during counseling who becomes hyperarousal needs various help to manage his or her emotions within the session. These skills and techniques can help not only help them regulate and expand the window of tolerance in session but also be applied later to out of session in the world experiences. The two most common types of skills taught in counseling for individuals with unresolved trauma and PTSD are grounding and containment.

Grounding techniques can be sensory, cognitive or somatic in nature. In sensory grounding, the counselor utilizes the five senses to help a survivor find placement in the present. In regards to the sense of touch, it can be as a simple as feeling the feet on the ground or the soft touch of the couch on the finger tips. A counselor should help the survivor with calming words describing the sensation one feels as the fingers sway across the texture of the couch, or the firm feel of the foot against the hard floor. In some extreme cases, ice in a person’s hand can be used to help a person find the present. In all cases, the sense of touch should be used especially carefully when counselor or client come into contract via a tap on the shoulder or a hug because these things could possibly be a trigger to the prior abuse (Compton, 2024, p. 214). With sight, the counselor can direct the client to note anything in the room they see and what color it may be or details one may not have noticed before. The scent of smell can help calm through oils, incense or candles that can help a person find calm but again be aware of your client’s history and scents that could trigger him or her. With taste, sometimes, one can focus on a piece of candy available and the taste of it, or imagine a particular dessert. The counselor gently inputs into the mind these scenes to help the client find regulation (Compton, 2024, p. 212). From a cognitive approach, a counselor can have a client count from a higher number down to zero to exert awareness of the now or have the client name things within the room to help the person find connection to the present. From a somatic approach, breathing exercises can be employed to help grounding. In fact, breathing exercises are sometimes the first utilized to help a person calm. Deep breathing initiate the parasympathetic nervous system which reverses the affects of the fight or flight response. The deep inhale and exhaling can lower the heart rate and help a person find calmness. Usually the breathing is done with some type of visualization. One common theme is balloon breathing where the client is told to imagine a balloon inside oneself and as one inhales to imagine the balloon inflating and while exhaling to imagine the balloon deflating (Compton, 2024. p. 212). The breathing should be coming from the abdomen and not the chest since chest breathing is usually associated with anxiety. To ensure proper breathing, one can tell the client to put his or her hand on ones chest and stomach and see which part of the body is moving more. One can also utilize touching the shoulders to see if the shoulders are rising which is indicator of chest breathing.
While grounding helps a survivor find the present and remain engaged, containment skills can help clients learn to control uneasy emotions. The tool of containment helps clients break away from traumatic memories and feelings (Compton, 2024, p. 215). Containment tools include visualization and various expressive arts. Most of these tools are also utilized with breathing techniques and can be used in session as well as in the real world. When working with clients expressive arts are similar to play therapy with children. They can help a person find calm when discussing difficult issues. Compton references vertical regulation as way for the survivor to draw lines of different colors up and down a page while deep breathing. Other expressive arts include dance and music to help with hypoarousal to push energy into the person. Liturgical or spiritual music can be utilized if it provides the necessary calm, or secular music that the client enjoys (2024, p. 211). Creative writing is another expressive art used to contain emotion. In expressive writing, one can write a note to oneself, or a parent, or God, or anyone the client freely wishes to write too. The message can be a positive one that employs safety and security (2024, p. 212). Visualization and breathing remain one of the most used containment practices in sessions. With guided breathing and the visual scripts from the counselor, the client can visualize safe and secure places when facing trauma memories or uncontrolled emotions. One classic visualization technique is imagining the a container in which the client can put all the unwanted emotions into and cover with a lid. The counselor guides the client to understand that any intrusive thoughts at any time can be stored in this container, box, or chest when needed (Compton, 2024, p.216). The key is to discover a safe, secure and calm place. Many times counselors will lead a guided visualization of a place the client finds peaceful. Whether a cabin in the mountains, or a spot on the beach, the counselor can take the client back to that place or peaceful place in time. During which the client will close his or her eyes, breath deeply and follow the voice of the counselor describing the calm associated with these places and times. Butterfly hugs are also a tool that can be utilized during visualization in which the client is taught to hug oneself and allow their hands to tap their back in assurance and calmness (Compton, 2024, p. 217).
In all of these exercises, if the person is spiritual or religious, spiritual aspects and words can be utilized on a case by case basis to help the person find calm. For some, spirituality may be beneficial but for others who were exposed to spiritual abuse, it may not be warranted. If spirituality is accepted and desired, sometimes clients can breathe in with a statement about God and breathe out with a statement of safety, such as “God is good” and “I am safe”. In other cases, scriptural references that the client enjoys can be utilized from whatever sacred book he or she adheres to (Compton, 2024, p. 218).
In all cases, help the client be in control. The purpose it to help the client learn to regulate and being in control is key, especially when the survivor is not in session. In such cases, when introducing breathing techniques or new tools, instead of dictating, or saying “do this”, utilize phrases such as “would this be helpful to do this?”. This reduces distress and gives autonomy to the survivor who in many cases, if abused, was told what to do numerous times.
Conclusion

Many situations in counseling trauma victims/survivors require helping them to learn to regulate emotions. These skills are important both in session and out in the real world. In session, it helps extend the window of tolerance which then can be applied to real world situations. Skills in grounding and containment help clients with hyper/hypoarousal and maintain control and learn to deal with the symptoms of trauma in a positive fashion. These tools in counseling also allow for the discussion, reflection and processing of the unresolved trauma. It is important to remember that when treating trauma, it is a marathon not a sprint. These skills take time to implement and the body and mind need time to heal.
Please also review AIHCP’s Trauma Informed Care Program, as well as its many healthcare certifications in crisis intervention, grief counseling, stress management and Christian spiritual counseling. All programs are open to qualified healthcare and mental health professionals seeking four year certifications to utilize within the scope of their practice. The healthcare programs are online and independent study and have mentorship as needed.
Resource
Compton, L & Patterson, T (2024). “Skills for Safeguarding: A Guide to Preventing Abuse and Fostering Healing
“Hypo-Arousal and Hyper-Arousal: Nervous System Dysregulation”. (2025). Mindset Explained. Access here
“Feeling Hypo or Hyper Aroused How to Spot the Subtle Signs”. (2025). Echowave. Access here
Additional Blogs from AIHCP
PTSD-click here
Counseling Clients through Crisis, Danger and Harm-click
Additional Resources
“13 Grounding Techniques for When You Feel Overwhelmed”. Cleveland Clinic. Access here
Schuldt, W. “Grounding Techniques”. Therapist Aid. Access here
Sutton, J. (2022). “7 Best Grounding Tools and Techniques to Manage Anxiety”. PositivePsychology.com. Access here
Caporuscio, J. (2024). “Step-by-step guide on grounding techniques”. Medical News Today. Access here
Gale, A. (2025). “Hyperarousal vs. Hypoarousal”. Carepatron. Access here
Alpern, P. (2025). “Is the freeze response a form of hyperarousal or hypoarousal?”. The Trauma Journal. Access here
“Feeling Hypo or Hyper Aroused How to Spot the Subtle Signs”.