Suppose there is an elderly patient who comes in repeatedly for minor falls. Strangely, all their test results are normal each time. It’s only later that the elephant in the room is addressed. The dim hallway lights at home and the fear of using the bathroom at night had contributed to most of their injuries.
Then there is another senior who shows promising signs of improvement, not after a change in their prescription medicines. What they needed was help with transportation and meal services.
All these scenarios have at least one thing in common, and that is how older adults seldom struggle with a single medical issue. Holistic care is nowhere more important than in geriatrics.
Since physical health, emotional stability, and social support are all connected, it’s important to understand how to deliver holistic care. This article will share four practical ways healthcare professionals can extend holistic care to senior patients.
Assess Comprehensive Patient Needs
How can the care be called holistic if it does not involve a thorough, multidimensional assessment of each senior patient? Besides physical health, healthcare providers must evaluate emotional, social, and environmental factors that influence overall well-being.
When all such needs are identified early, it’s possible to design interventions that are truly patient-centered. A key part of this assessment has to do with understanding VA benefits for seniors.
The Department for Veteran Affairs enables healthcare professionals to connect eligible patients with healthcare programs, mental health support, and community resources. The VA Pension for Senior Veterans provides monthly financial support to low-income wartime veterans who are above 65 years.
It covers daily expenses so seniors can maintain their independence. Awareness of provisions like the one mentioned above ensures that patient care plans address both medical and social determinants of health. On that note, listed below are the steps for a thorough patient assessment:
A comprehensive health evaluation, which includes reviewing chronic conditions, medication management, and fall risks
Psychosocial assessments that check emotional health, potential stressors, and social support networks
Proper documentation that is later integrated into the care plan, ensuring follow-ups and interdisciplinary collaboration
Unless all dimensions of a senior patient’s life are examined, it isn’t possible to develop personalized and sustainable interventions. Then, how will patient satisfaction and long-term outcomes change for the better?
Collaborate With Interdisciplinary Teams
Teamwork is often seen as the cornerstone of a strong organization. The same holds in the case of a healthcare institution, where collaboration has been prevalent since the 1960s. Especially since we are talking about holistic care for senior patients, clinicians who work as part of a coordinated interdisciplinary team enhance patient outcomes.
This happens due to increased patient safety and lower risk of complications/medication errors. Nurses are often the primary communicators in such teams. They help to bridge clinical needs with support across social, functional, and psychosocial areas. That’s a critical role because many senior patients suffer from multiple conditions at once.
In a 2025 observational study conducted on patients over 65 with multimorbidity, it was found that interdisciplinary care programs reduced conventional hospitalizations by 45%. Even emergency visits and outpatient encounter numbers went down compared to the year prior. This means collaboration does have real value.
However, it is important to ensure that collaboration takes place the right way. Key elements of it include:
Periodic communication through reviews or team huddles that keeps everyone on the same page
Proper development and updating of a shared care plan to ensure every provider understands the patient’s overall goal
Role clarity and accountability that reduce the chances of duplication, as well as ensure essential tasks are completed
Collaborative problem-solving to overcome barriers and prevent challenges from turning into adverse events
Interdisciplinary collaboration may be the only way in many cases to maintain continuity and efficiency in senior care.
Support Mental and Emotional Well-Being
It’s no longer a secret that mental health directly affects physical well-being. Unresolved emotions have their way of accumulating stress in the body. When chronic, the stress translates into inflammation that disrupts normal bodily functions.
In 2024, around 33% of adults between the ages of 50 and 80 years reported feeling lonely sometimes or often in the previous year. Nearly 29% also admitted to feelings of social isolation. The situation was bad enough to affect health outcomes.
Besides being uncomfortable, such feelings are linked to poorer physical health and a higher risk of anxiety/depression. These factors can complicate clinical care if left unaddressed. This means focusing on emotional well-being is crucial to providing comprehensive, patient-centered care for seniors.
So, what can some practical strategies be? They are as follows:
Make routine mental health screening a must for every senior patient.
Connect patients with counseling, therapy, or community programs to reduce isolation and increase engagement.
Encourage participation in group activities, volunteering opportunities, etc., to strengthen social ties.
Teach patients stress-reduction techniques, including mindfulness, deep breathing, and relaxing exercises that support emotional regulation.
Practice empathy during communication through active listening and validation to make patients feel heard and respected.
Promote Patient Empowerment and Education
Earlier, there existed a patriarchal doctor-patient relationship, one that has started changing now. Today, there is an equal-level partnership that involves patient autonomy. In other words, patients have started contributing to their care with rich insights, data, preferences, and whatnot.
Is digital health responsible for driving such a promising turn of events? Perhaps, plus, self-management is the cornerstone of holistic care. This doesn’t change just because of a patient’s age. Clinical treatment is essential, but outcomes improve when the senior can understand their own health and participate in care decisions.
As per a 2025 report, 83% of primary care users aged 65 and above with at least one chronic condition reported their social functioning to be good or excellent. This study was conducted across 17 OECD countries, highlighting that most older adults are capable of maintaining active social roles when supported.
Since a considerable minority still struggles, it all boils down to patient education and empowerment. Here are some effective ways in which healthcare professionals can promote both:
Extend tailored education by personalizing explanations about medications and disease management to each senior’s literacy and preferences.
Teach concrete skills related to diet adjustments and recognizing early warning signs.
Point patients towards local programs, workshops, and services that facilitate active engagement.
Include family members in care discussions (with consent), so they can also support the senior’s daily routine.
Involve the patient directly in the process of setting health goals and care plans to boost their confidence.
If there was ever a time that demanded holistic care for seniors, it is now. Statista shares that 24% of older adults reported their general health as fair or poor in 2024.
This shows that nearly one in four seniors continues to face major health challenges the further they age. With holistic care measures, nurses and licensed healthcare professionals can enhance quality of life, not just health. Aging was never meant to be reduced to crisis management, and holistic care understands that fully.
Author Bio:
Agwalogu Bob holds a Bachelor’s degree in Economics and has been crafting high-performance content since 2017.
He has worked with some of the world’s leading content agencies in the UK, Ukraine, India, and Nigeria, producing engaging copy in the SaaS, finance, tech, health and fitness, and lifestyle niches.
When he’s not working on a project, you’ll likely find him trawling the internet for funny memes. You can connect with Bob on LinkedIn or via The List Hub.
Please also review AIHCP’s Holistic Nurse Certification program and Holistic Care Courses see if it meets your academic and professional goals. These programs are online and independent study and open to qualified professionals seeking a four year certification
A slip doesn’t mean falling short. For countless individuals dealing with addiction or persistent emotional struggles, setbacks pop up often. They’re expected, even anticipated. Despite careful effort, some faces carry greater weight; those closest to the crisis tend to vanish from attention first. After a setback, people sometimes skip future appointments, drift away from treatments, or stop showing up altogether. Instead of seeing it as nonadherence, there could be recognition – the environment might have failed them badly along the way. One reason some patients at high risk for relapse often slip through the system isn’t that they don’t care – it’s how care systems actually work. Care shifts outside hospitals, yet support often vanishes when patients re-enter daily life. Hidden roadblocks, like a lack of follow-up or access to services, play a bigger role than most assume. When these pieces don’t fit together, staying sober gets harder, no matter how much someone wants to comply.
High-Risk Patients Need More Than Short-Term Stabilization
Most recovery approaches aim only at stopping crises, not long-term care. Someone shows up struggling, gets strong help for a few weeks, then leaves after things start looking better. It may be marked as an achievement. Right after leaving treatment, things can feel shaky – this is when setbacks often creep in.
Out there, patients at high risk for relapse usually move from hospital care or set programs into a new routine meant for stable situations. That might come with scheduled counseling, taking drugs as needed, sharing with others going through similar things, plus adjustments to daily habits. The real question, however, is how likely someone is to stick with it once they leave controlled ground? Getting around, job hours, looking after family, plus money worries – these make it hard to stick with treatment. If nobody keeps track after everything is set up, good intentions often fade fast.
Risk often stops being checked once someone leaves the hospital. Even if a person seems stable after treatment, hidden stressors remain – like ongoing hardships or weak connections with others. Without regular follow-up, small red flags go unnoticed. By the time someone finally returns for treatment, the problem can be quite serious.
Systemic Barriers and Treatment Gaps That Push Patients Out of Care
What often goes unnoticed is how the way health care is set up can lead patients at high risk for relapse back into old habits. Moving from one kind of support to another isn’t always straightforward – the pieces rarely fit together well. After finishing detox or staying in a hospital-based program, waiting months for follow-up sessions can feel like hitting a roadblock. Coverage shifts happen, doctors sometimes stay silent, while promised visits vanish into thin air. This is the reality of finding appropriate care for many high-risk patients. Before steady help arrives, frustration piles up, pulling people away before anything truly takes hold.
Getting care often poses a serious hurdle. Out in the countryside, people can find almost no doctors nearby. Meanwhile, city residents face an opposite problem with waiting lists stretched thin, and spots for expert treatment vanishing fast. Most commonly, help comes through telehealth, yet problems remain – many people lack steady internet or quiet places to meet online. When communication clashes or group norms carry judgment, taking part gets harder still.
Fixing these flaws takes effort. Evidence shows that warm handoffs between providers significantly reduce dropout rates. Planning post-hospital visits ahead, say during treatment, cuts down on lost steps later. Within a week of leaving the hospital, those who hear back soon tend to stay out of trouble and avoid another stay. Expanding care coordination roles, integrating behavioral health into primary care, and using shared electronic records are practical steps that reduce fragmentation and keep patients connected.
Patient-Level Challenges Are Often Misunderstood
What often goes unseen is how people struggling to stay sober deal with deep underlying issues. Trauma and mental health problems, together with stress, can quietly lower drive and clarity over time. Expecting someone like that to manage themselves well ignores what pain does behind closed doors.
Money troubles play a role, too. Coverage through insurance helps, yet still, co-payments, drug prices, plus wages sitting untouched build fast totals. Facing that hard moment, where care clashes with food or shelter, people tend to pick survival above all. What looks like a refusal to accept help might simply be how people act when supplies run low.
Social isolation can play a huge role, too. When you don’t have friends around, or they’re always at places that allow and encourage drug use, your temptations might never fade. Lack of support from others close by, from the healthcare professionals, or the community at large, makes staying on track far tougher. Studies keep finding the same pattern – people with solid social networks tend to stay healthier in recovery. Still, most programs act like support is a bonus, not a must.
Risk Assessment Often Stops Too Soon
Few realize risk assessment is something that should be continuous, not just happen once at the beginning of the process. At first glance, some patients seem risky; yet those warnings rarely change how treatment is given later. When symptoms fade, attention tends to drop too – while danger could still burn bright underground. Luckily, most clinics have methods to monitor warning signs, but these stay forgotten or used unevenly. Shifts in how someone sleeps, handles pressure, or sticks to pills often hint at growing danger – though records might miss them between appointments. Sometimes people hide concerns because they worry they’ll be judged harshly or face loss, like a home or job.
Looking closely at risks often feels clearer if done alongside steady talks and feedback. If patients see trouble as an opening for help instead of a loss of care, they tend to speak freely. Research indicates tracking signs like mood or behavior over time helps treatment work better and catch issues sooner. Long-term data show why ongoing assessment matters. Looking back ten years, people who dealt with both mental illness and drug issues saw frequent returns of symptoms, even long past their first help. When follow-up ends or weakens, setbacks grow more likely. This reinforces the need for relapse risk to be treated as dynamic, not something that can be ruled out after early improvement.
Continuity of Care Requires Accountability Across the System
It’s easy to say recovery depends on one person. However, responsibility shouldn’t stop at the patient. When help doesn’t come through, when appointments slip, or when teams fail to share updates, patients are those who pay the price. Shifting focus this way leads less to steady progress, more to repeated hospital visits.
However, when there’s clear accountability and all the responsibilities are spelled out, things run more smoothly. A named contact – either person or team – watching over aftercare keeps patients from slipping through cracks. That is how healthcare professionals can support better rehab outcomes. When main clinicians, mental health staff, and outside helpers all line up around one unified plan, progress doesn’t get lost between visits.
What happens behind the scenes shapes outcomes, too. Setups pushing quick check-ins and repeated customer flows rarely allow deep connections. When success is tied to results, not just numbers, caregivers tend to focus on stopping problems early and staying in touch later. Early data from integrated care programs show reductions in relapse-related hospitalizations and overall costs.
Practical Strategies That Reduce Relapse Risk
There’s no one answer that can fix everything, yet a few methods keep bringing results. Right after treatment, reaching out soon – often before days pass – makes a difference. Checking in early, maybe by stopping by, calling, or sending a note, helps keep ties strong while handling small problems as they arise.
Another point: care plans must have a good understanding of addiction and take into account actual daily challenges. Think flexible schedules, straightforward medicine directions, and unexpected cancellations covered ahead of time. Good care doesn’t drop rigor – it removes what blocks progress. Another point is that peer support, along with group efforts in the community, fits well within organized care systems. People who’ve gone through similar struggles – called peer specialists – often bring unique insight when working alongside professionals. Because they understand challenges firsthand, their presence tends to strengthen both continued involvement and overall experience. Finally, what matters most is how systems handle information ahead of time. Watching out for canceled visits, skipped meds, or shifts in symptoms gives staff a chance to step in before things worsen. When applied responsibly, data forecasting might show which patients require extra attention instead of reacting too late.
Moving From Blame to Prevention
Patients at high risk for relapse do not slip through the system by accident. Cracks in care, misplaced hope, and spotty checks let problems pass unchecked. Seeing it clearly means naming what goes wrong instead of pointing fingers. Even though setbacks happen for certain individuals, multiple repeat episodes shouldn’t happen regularly. If services truly mirror daily realities instead of ideal models, more will make it through challenging stretches without falling off track. In the end, it’s important to know relapse does not come from missing a moment. It grows when effort slips beneath routine. Stability hides risks the deepest. That is where support shapes what comes next.
Bio:Pam Reiman is a licensed clinical social worker and addiction specialist with extensive experience in behavioral health and dual diagnosis care. With a background in both law and clinical practice, she focuses on improving treatment access, care coordination, and long-term recovery outcomes for high-risk patients.
References:
Waite, M. R., Heslin, K., Cook, J., Kim, A., & Simpson, M. (2023). Predicting substance use disorder treatment follow-ups and relapse across the continuum of care at a single behavioral health center.Journal of Substance Use and Addiction Treatment, 147, 208933. https://doi.org/10.1016/j.josat.2022.208933
Xie, H., McHugo, G. J., Fox, M. B., & Drake, R. E. (2005). Substance abuse relapse in a ten-year prospective follow-up of clients with mental and substance use disorders.Psychiatric Services, 56(10), 1282–1287. https://doi.org/10.1176/appi.ps.56.10.1282
Please also review AIHCP’s Case Management Certification program and Case Management Courses see if it meets your academic and professional goals. These programs are online and independent study and open to qualified professionals seeking a four year certification
Counseling looks to help people change for the better. Habit in either direction is wired in our brain and it can be a difficult journey to incorporate good change. This video takes a closer look at a change and the process
Fritz Pearls and his wife are considered the pioneers behind the development of Gestalt Therapy and its numerous techniques. While, like many numerous systems, Gestalt by itself is limited by its own definitions and guidelines, but still nonetheless has supplied the counseling sciences with numerous theories as well as practices to aid counselors in helping people. Pearls, a German immigrant, spent most of his later lifetime in the USA, developing and implementing the concepts of Gestalt. It remains to this day an original way to help individuals face psychological issues and pursue change.
Gestalt focuses on the here and now and awareness of one’ internal and true emotions. Please also review AIHCP’s Behavioral Health Certifications, especially in Grief Counseling
Please also review AIHCP’s numerous Behavioral Health Certifications, including Grief Counseling, Christian Counseling, Trauma Informed Care, Crisis Intervention, as well as Stress Management, ADHD Consulting, Anger Management, Clinical Hypnotherapy, EFT, and Meditation.
Gestalt Therapy
Gestalt is very focused on the now of the person. It sees current problems in how individuals hide behind their issues and avoid them. It is less concerned with issues of the past but how more so the person deals with the now and how that person transforms. It is very person centered in finding the answers in the client but unlike classical person centered therapies which has a more gentle guiding approach, Gestalt employs more direct confrontation when necessary to push a person in facing oneself in the present. Like most person centered therapies, Gestalt feels the power of change and how to live resides in the subjective reality of the person and that when a person accepts who he or she is and faces the illusions of self and takes responsibility for oneself, then one can become free and have a more healthy mental life. In this way, Gestalt looks at the wholeness of the person and challenges the person to self awareness. It is because of this approach, Gestalt is immersed in the human experience and how life is experienced. In its concern of the here and now, as well self awareness, it is more concerned with the question of how than the question of why.
Utilization of Gestalt
Pearls utilized exercises and experiments as the way to help clients find self awareness. Exercises helped clients experience the now of emotion, but experiments were deeper techniques to help a person become self aware and challenge oneself. Many of these experiments employed by the therapist was utilized as ways for the client to become self aware and how to properly express oneself to find balance with one’s inner voice. In many cases, Pearls would identify acts of phoniness by a person due to external pressures that subdued the internal personality of a person. He would note how one’s tone of voice, or facial expressions, or body postures would not match the feeling internally. He utilized various exercises and experiments to help the person break free of these uncomfortable anxieties and to better express oneself.
Gestalt therapy challenges a person to be more self aware of how the person feels
Pearls employed various linguistic alterations to a person’s vocabulary or how the person stated something in therapy. This involved utilizing personal pronouns more in the client’s speech. Instead of making a statement that was void of personal need, Pearls would instruct the person to utilize the pronoun “I” to own the statement. Instead of a passive declaration of what one desired or wanted or disliked, Pearls instructed the client to say “I need, or I want, or I dislike”. In addition, he removed such contractions as “can’t” to “won’t”. Instead of stating I cannot do something, he pushed clients to say I will not do something. Also, instead of the conjunction “but” used to imply an excuse, he instructed clients to use the word “and”. For example, if someone has a paper to write and states “I cannot write the paper tonight, but I may try to do it tomorrow”, Pearls would have the client transfer the statement to “I will not write the paper tonight and I will try do it tomorrow”. Pearls also would emphasize the use of the phrase, “I take responsibility for this”. Hence a person would say “I take responsibility for not writing the paper tonight”. This clearly shows an emphasis of owning one’s inner feelings more deeply and also expressing what one wants in a more authoritative, responsible and personal way. Excuses, passive language and not asserting one’s own needs into a sentence were signs of the person not being self aware of what one needs and not taking responsibility for it. Hence, Pearls was less concerned about other pronouns of “them” or “us” or how others make one feel but more interested in how oneself makes one feel.
In addition to speaking with more authority and emphasizing responsibility for one’s words, thoughts and actions, Pearls would help individuals identify body posture, nervous ticks, or uncomfortable laughs as the ways the body and its physiology would manifest discord between expression and the actual feeling. Pearls would frequently call a person out with confrontation for expressing oneself in contradiction to how one felt. He would suggest exaggeration of these tics, or tones, to see how truly silly or phony they were in contrast to how the person felt in the moment. Through the experiment of exaggeration, Pearls encouraged one to bite one’s lip harder, or tense their jaw more pronounced so that the person could recognize these manifestations when internal feelings emerged. The key for Pearls was to help the client discover and become aware of one’s deeper feelings in the now moment and how to properly communicate and express them. This involved analyzing one’s own bodily reactions in correlation with the feelings internally.
The most famous experiments of Pearls was the empty chair. This created an opportunity for one to confront oneself, or another in the safety and privacy of therapy. It permitted one to become aware of self, but also to express emotions that may have been kept in check. The first usage of this experiment was direct dialogue between self. For example, a middle age man may have many regrets in life and has two images of himself; namely the driving and commanding side of himself and then the more relaxed version of self. At direction of the therapist, the man would move from his chair to the other chair and imagine speaking to himself in a more authoritative way. In response, the man then would remove to his original chair and respond to his more aggressive and demanding side. This dialogue would continue to until the man discovered his many needs. In other cases, the empty chair can be utilized as a way for an individual to confront another person. This may be an ex spouse, a parent, a boss, a deceased family member, or even God. The client is encouraged to speak to this person if as the person was truly sitting there. Obviously this is an advanced therapeutic tool and should be conducted by a trained therapist due to emotional eruptions that can occur. Pearls saw this as a way for a person to truly express one’s emotions without filter or restraint free from possible danger of physical confrontation.
Conclusion
Please also review AIHCP’s numerous behavioral and healthcare certifications
Gestalt has many beneficial applications to help people properly express their feelings, be aware of themselves and become more connected to how they truly feel. It is beneficial for those suffering from anxiety as well as depression. However it does possess some limitations. It is more emotional in nature and does not give enough attention to the intellectual and cognitive issues surrounding mental health. It also focuses more the now without less concern for the past. Questions such as why and what are more replaced with how can we handle this now. It is also weighs heavily on one’s own personal needs for self actualization and less concern for the needs of others. This is a double edged sword if not properly put into context. Further, it possesses a more subjective morality in place of universal objective standards of behavior or morality. Yet, many of its experiments and uses are widely accepted and utilized in daily practice. Very few counselors completely adhere to one particular school over another, so the percentage is quite low of a counselor being a strictly Gestalt therapist. Most modern day counselors share Gestalt techniques and implement them with person centered therapies and behavioral therapies for maximum results.
We explore the practices of early Christianity to see major theological developments that shaped the faith over centuries. The observance of Lent is a key part of Christian tradition and prepares believers for the celebration of Easter. This season of reflection and penance asks believers to examine themselves, fast, and pray. These actions mirror the 40 days Jesus spent in the wilderness. The history of Christianity from its start through the Medieval period explains how Lent developed within different cultural and theological settings. Also, the study of catechesis in the early Christian era shows the link between teaching and understanding. This is especially true regarding the role of Lent as a time for spiritual growth and renewal. We examine these basic elements to see how Lent shapes individual lives and strengthens the shared identity of Christianity.(Dr. Arnold R, 2017). Additionally, the study of catechesis during the early Christian era highlights the relationship between teaching and understanding, particularly concerning the significance of Lent as a time for spiritual growth and renewal (Fogleman A, 2023). By examining these foundational elements, we can gain a deeper appreciation for how Lent not only shapes individual lives but also fortifies the communal identity of Christianity itself.
Lent is time to allow Christ back into one’s heart
Lent is a profound season of reflection and spiritual renewal within Christianity. It traditionally spans 40 days leading up to Easter. This time features practices like fasting, prayer, and almsgiving. These acts aim to deepen the believer’s relationship with God. Lent has a dual function. It prepares the faithful to celebrate the Resurrection of Christ at Easter. It also reminds them of the journey toward redemption and renewal. Believers confront their vulnerabilities and sinfulness during this season. They relinquish self-reliance for divine grace. They recognize that human efforts alone fall short of God’s promise of a full life. This duality appears in the teachings of N. Fedorov. He connects Lent with the philosophy of active Christianity. He notes the transformative potential of Easter as a symbol of hope and renewal.(McCarthy A et al., 2020)(Anastasia G Gacheva, 2020).
The historical origins of Lent trace back to the early Christian church. The church wanted to prepare believers for Easter through reflection, penance, and fasting. Initially, the practice began as a way to replicate the 40 days Jesus spent fasting in the desert. It provided a structured time for spiritual discipline. This period held great meaning as a communal effort to understand Christ’s suffering and resurrection. Lent became a formal observance by the fourth century. Practices varied across different regions, and this showed the diversity within early Christianity. Scholars argue that these practices evolved alongside broader trends in the early Christian movement. They reflect the interaction of faith and tradition (). The complex development of Lent illustrates the church’s growing liturgical structure. It also shows the shift from personal fasting to communal observance. This highlights the major role of Lent in shaping Christian identity ().(Burton L Mack, 2023)). The complexities of Lents development illustrate not only the churchs growing liturgical structure but also the gradual shift from personal fasting to communal observance, underscoring the significant role of Lent in shaping Christian identity ((Dr. Arnold R, 2017)).
The study of Lent remains relevant in modern society. It invites people to think about personal growth, discipline, and spirituality. This season urges believers to examine themselves and repent. They build a better grasp of their faith and moral values. Such deep thought is necessary. The world is full of unclear ethics and moral relativism. Habits like fasting and prayer balance against social pressures. Individuals gain strength and clear purpose. Lent also has meaning in schools. Its moral lessons guide talks on ethical habits. This includes problems with exam cheating. Studies show that faith aids personal growth and school grades. They note the value of matching lessons with deep beliefs. Understanding Lent improves spiritual and ethical life. It helps in a complex world.(O Olabode, 2019). Studies also highlight how faith-based approaches can enrich personal development and academic performance, stressing the importance of aligning educational content with deep-seated beliefs (Miller PT, 2024). Consequently, understanding Lent can enhance both spiritual and ethical dimensions of life in today’s complex landscape.
The Bible bases Lent on themes of repentance, fasting, and spiritual renewal. Many scriptures show the value of these habits. They stress the need for self-examination and humility before God. Jesus fasted for forty days in the wilderness. This event acts as a central model for Lent. It shows the spiritual strength that comes from self-denial and prayer. This time of reflection reveals human brokenness. It points to the need for divine grace. We try to be righteous on our own. Yet, our efforts are never enough. Christians participate in Lent to mirror Christ’s sacrifice. They also embrace the life promised in the Paschal mystery. This season prepares believers for the celebration of Easter and the deep joy of the resurrection.(McCarthy A et al., 2020). Christians engage in Lent not only to replicate Christ’s sacrifice but also to embrace the fullness of life promised in the Paschal mystery, highlighting that the journey through Lent ultimately prepares believers for the celebration of Easter and the profound joy of resurrection (Budnukaeku AC, 2024).
Christians enter the Lenten season. They draw inspiration from scriptures that explain their practices and beliefs. This time involves themes of sacrifice, reflection, and renewal found in the Bible. Matthew 4:1-11 calls for repentance and humility. Jesus fasts for forty days in this passage. It serves as a model for Christians who want to deepen their faith during this period. Other texts discuss human frailty and divine grace. These writings remind believers to rely on God for redemption. They express reflections on brokenness and a need for divine fulfillment. People recognize that personal efforts alone cannot fill spiritual voids. They accept the power of God’s grace. This leads to the joy and hope of the Easter resurrection. This pattern of sacrifice and celebration is central to the Lenten experience. [cite1] and [extractedKnowledge1] highlight the theology behind these practices. They help create a deeper connection to the Christian faith.(N/A, 2023) and (McCarthy A et al., 2020) underscore the profound theological underpinnings that guide Lent practices, facilitating a deeper connection to the Christian faith.
III. The 40 days of fasting and Jesus’ temptation in the wilderness
Christ was tempted for 40 days and emerged victorious over Satan. Through Christ’s example and grace we can also emerge victorious after Lent
Jesus spent 40 days fasting in the wilderness and faced temptation there. These events serve as the foundation for Lent in Christianity. This fasting is an act of self-denial. It also symbolizes the spiritual preparation believers need for penance and renewal. Jesus faced temptations in the wild that challenged His divine mission. This showed human vulnerability and the need for strength from God. The story reveals the difficulties of faith. Individuals try to overcome personal failings while facing outside pressure. These struggles mirror the experience of Lent. Christians fast and reflect during this season. They remember their own brokenness. They see that God’s grace is necessary for true fulfillment. The context of fasting in the New Testament is also important. It offers a complete view of the practice. This knowledge highlights spiritual discipline and helps people grow closer to God.(McCarthy A et al., 2020). Furthermore, understanding the context of fasting within the New Testament provides a holistic view of its significance, highlighting both the spiritual discipline and its potential for fostering a deeper relationship with God (Steven H Mathews et al., 2013).
The season of Lent is a preparation period for Christians. It establishes a strong connection to the Passion of Christ. This connection includes His suffering, crucifixion, and resurrection. Lent relies on reflections regarding Jesus’ trials. It asks believers to perform acts of penance and self-denial. These acts mirror the sacrifice in the Gospel narratives. The symbol of the cross is a central focus during this time. It represents Christ’s agony and the promise of redemption through His sacrifice . The meaning of Jesus’ trials before authorities adds to this bond. These trials highlight the injustices He faced. They help explain human suffering and divine love . Christians emulate Christ’s sacrifices during this season. They prepare to celebrate the victory of His Passion at Easter. This marks the importance of this time.(Banna YE, 2024). Furthermore, the theological implications of Jesus trials before the authorities deepen this connection by highlighting the injustices He faced, which serve as a blueprint for understanding human suffering and divine love (Rev. Dr. Reumann JH). Thus, as Christians undertake their Lenten journey, they not only emulate Christ’s sacrifices but also prepare to celebrate the victorious culmination of His Passion during Easter, marking the significance of this transformative season
IV. Practices and Traditions During Lent
Lent is a time for reflection and spiritual renewal. It features many practices and traditions with deep meaning in the Christian faith. Fasting is central to Lent. This practice leads believers to give up certain luxuries or foods. They do this to rely more on God. This sacrifice asks people to face their human vulnerability. It highlights a key truth. Sincere efforts fail without divine help. The season leads toward Easter and the happy celebration of resurrection. It reminds believers of God’s promise to overcome human weakness. Rituals include prayer, almsgiving, and communal worship. These acts build a sense of community and shared faith during this season of change. Scholars study the complex link between these rituals and early Christian beliefs. They see how these traditions united communities in the growing Christian movement.(McCarthy A et al., 2020)(Katrine A de Gudme H et al., 2018).
The practices of fasting, abstinence, and penitence are central to observing Lent in Christianity. They serve many spiritual purposes. Fasting traditionally means staying away from specific foods or meals. It represents a period of self-denial that aids contemplation and spiritual growth. This discipline rests on a belief that people can build a stronger connection with God through restraint. Similar intentions appear in other traditions like Islam. There, fasting controls desires and builds a sense of community (). Abstinence during Lent often involves giving up luxuries. This highlights the value of sacrifice and reflection. Believers can then reset their priorities toward faith and morality. This process of penitence is about more than the physical act. It represents a commitment to spiritual renewal. It reveals the changing nature of religious teachings. These teachings evolve across cultures ().(Mansor NH et al., 2022)). Additionally, abstinence during Lent, often from luxuries or specific pleasures, emphasizes the importance of sacrifice and reflection, allowing practitioners to realign their priorities towards faith and morality. This journey of penitence is not merely about the physical act of abstaining; it embodies a broader commitment to spiritual renewal and transformation, revealing the dynamic and contextual nature of religious teachings that continue to evolve across cultures ((Alfian A, 2022)).
Fasting according to most schedules is a act of self control to teach the passions and curb inclination to sin. Fasting is more severe penance of Lent and occurs officially on the Church calendars in both East and West only twice. The first day of Lent and Good Friday. In the West, this involve no meat, and only one full meal with 2 smaller meals that equal one meal. There is no eating in between these times. Fasts are required from ages 18 to 59 for most church disciplines with dispensations for hard laborers, as well as the sick or elderly or those with health conditions. In the East, the fast is merely no meat and dairy. Days of abstinence involve no meat only and occur every Friday in the West and every Wednesday and Friday in the East. Those who wish to fast more or abstain more are welcome to go beyond the minimum regulations of the Church, but are encouraged to give something up, or practice some type of sacrifice in their personal life.
Prayer, fasting and repentance are key callings during Lent. Please also review AIHCP’s Christian Counseling Certification
In Christianity and Lent, prayer and spiritual reflection are critical. They guide the faithful through repentance and renewal. During Lent, believers pray more deeply. This creates a connection with God that goes beyond simple ritual. This introspection asks people to consider their spiritual state. They recognize the need for divine grace and healing. Modern literature shows that combining faith with reflective practices improves the care one provides. This applies to spiritual mentorship and other professions. The Lenten experience also highlights the two sides of human existence. People face blessings and brokenness at the same time. This tension pushes believers to give up self-reliance. They seek fulfillment through God. This reflects the call to accept divine help over personal achievement. Prayer and reflection during Lent lead to spiritual wholeness.(Camden L Baucke et al., 2022). Furthermore, the Lenten experience underscores the duality of human existence—the simultaneous blessings and brokenness faced by individuals. This tension compels believers to surrender their self-reliance in favor of seeking fulfillment through God, reflecting the call to embrace divine assistance over personal achievement (McCarthy A et al., 2020). Thus, prayer and reflection during Lent cultivate a transformative journey toward spiritual wholeness.
Christians observe Lent and focus on almsgiving and charity. These acts deeply reflect their faith and dedication to the community. Believers see how their spiritual lives connect with the needs of others. They match personal sacrifice with compassion. Almsgiving is more than a simple obligation. It embodies Christ’s teachings. He commanded his followers to serve the marginalized in Scripture (Mat 25:40). This giving builds a better understanding of the joy of God’s Kingdom. That joy links to serving “the poor, the crippled, the blind and the lame” (Lk 14:3). Believers face the challenges of Lent. Their charity becomes a clear expression of faith. It shows that full life and grace are gifts from God alone. [extractedKnowledge1] and [extractedKnowledge2] note this truth.(McCarthy A et al., 2020) and (Morrison G, 2017).
V. Variations of Lent Observance Across Christian Denominations
Christian denominations observe Lent in different ways. These variations reflect specific theological views and liturgical customs. Roman Catholics typically fast, pray, and give alms. This leads to the celebration of Easter. This tradition connects to the Paschal mystery. It stresses spiritual change through self-denial and community service. Many Protestant denominations take a flexible approach. They focus on personal reflection and repentance instead of strict food rules. Some groups stress grace over works. They encourage believers to perform acts of kindness and charity rather than just fasting. Certain denominations add communal worship services to improve the Lenten experience. These services show a commitment to communion, participation, and mission. Each tradition approaches Lent with a unique focus. These differences make the Christian faith richer. They support diverse forms of devotion and spiritual renewal.(McCarthy A et al., 2022). Additionally, certain denominations may include communal worship services that enhance the Lenten experience, showcasing a commitment to communion, participation, and mission (McCarthy A et al., 2020). As each tradition approaches Lent with its unique emphasis, the variances deepen the richness of the Christian faith, fostering diverse expressions of devotion and spiritual renewal.
Roman Catholic Lenten customs
The Roman Catholic tradition treats Lent as a sacred time for penance, reflection, and spiritual growth. Distinct customs define this period for the faith community. The season begins on Ash Wednesday. People receive ashes on their foreheads to symbolize mortality and the call to repentance. This important practice has lasted for centuries. Believers fast, give alms, and pray more during these weeks. These acts show a communal understanding of sacrifice and devotion. The value of these customs goes beyond simple ritual. They build a deeper link to the wider story of Christianity and the time leading to Easter. Scholars note that these practices strengthen individual belief. They also create a sense of group identity among worshipers. These Lenten rituals also reflect old traditions in Church of England rites. This shows a shared heritage between different Christian groups.(Katrine A de Gudme H et al., 2018). Furthermore, the incorporation of rituals into the Lenten season reflects a longstanding tradition within the Church of England rites, demonstrating a shared heritage among various Christian denominations (N/A, 2021).
Eastern Orthodox Lent practices
Eastern Orthodox Christianity observes Lent with many spiritual practices and communal activities. In the Eastern Orthodox, Lent follows the Julian calendar instead of the Gregorian. This causes it to start earlier or later than the Western Churches with possible times when they both align. Like the Western denominations, the Orthodox encourage acts of repentance and renewal. Clean Monday marks the start of this distinct spiritual season. Believers engage in stricter fasting regulations and abstain from animal products. They also increase their prayer and charitable actions. These practices are rooted in the teachings of the Church Fathers. Figures such as Maximus the Confessor provide theological guidance. He emphasizes the transformative power of repentance and spiritual discipline. Groups like the Communities at New Skete adapt traditional practices for modern needs. This reflects an active approach to Orthodoxy in modern contexts. Dialogues between Eastern Orthodox and Protestant Evangelical traditions shape new understandings of Lent. These exchanges further enrich the spiritual environment. Lent becomes more than a period of fasting. It is a communal journey toward deeper faith.(Mettasophia et al., 2019). Additionally, the dialogue and exchanges between Eastern Orthodox and Protestant Evangelical traditions have begun shaping new understandings of Lent, further enriching the spiritual landscape (Nassif B). Through these practices, Lent becomes not only a period of fasting but also a communal journey toward deeper faith.
Protestant approaches to Lent
Protestant traditions treat Lent as a time for personal reflection, repentance, and spiritual renewal. This differs from the ritualistic practices in some liturgical denominations. Many Protestants believe Lent prepares them for Easter. They focus on individual accountability and a personal relationship with God. The season encourages believers to examine themselves. They practice disciplines like fasting, prayer, and almsgiving. These acts aim to help them grow spiritually rather than follow strict rules. Congregations often focus on reading Scripture and community service. This reinforces the principle that faith must show itself in action. Many Protestants find inspiration in the teachings of Jesus. They see Lent as a chance to follow His example of sacrifice and service (). This view highlights the value of self-denial. It also starts discussions about what discipleship means today ().(Zhong L et al., 2025)). This interpretation not only highlights the significance of self-denial but also invites discussions around the broader implications of modern-day discipleship ((Yan H, 2023)).
VI. Conclusion
The observance of Lent within Christianity acts as a time for reflection, self-discipline, and spiritual growth. This liturgical season invites adherents to explore their faith deeply. It leads to the celebration of Easter and the resurrection of Christ. The resurrection is foundational to Christian belief. Scholarship emphasizes the complex origins of resurrection Christology. This discourse reveals historical and theological dimensions. It also shows psychological factors. These factors influence how believers view scripture and faith practices (). Different psychological types interpret biblical texts in various ways. These interpretations show the variety of worship and understanding among Christians. This diversity is clear within Pentecostal traditions (). Lent provides a vital framework to examine personal and communal expressions of faith. It encourages Christians to engage with their beliefs actively. This connects them to the powerful message of Jesus Christ.(Loke ATE, 2020)). Furthermore, the diverse interpretations of biblical texts within the context of various psychological types illustrate the multifaceted nature of worship and understanding among Christians, particularly within Pentecostal traditions ((Leslie J Francis et al., 2019)). Ultimately, Lent stands as a critical framework for examining both personal and communal expressions of faith, encouraging Christians to engage with their beliefs actively and fostering a deeper connection to the transformative message of Jesus Christ.
During Lent we carry our crosses with Christ and prepare to suffer with Christ but also rise with Christ on Easter
Lent plays a central part in Christian spiritual life. It gives believers a set time for reflection, renewal, and growing in faith. This period lasts about forty days. It encourages Christians to take part in fasting, prayer, and giving alms. These acts build a deeper bond with God and help people accept their personal limits. [citeX] explains this dynamic. People often try to improve themselves through their own hard work. Yet true satisfaction comes only from depending on God’s grace. Admitting this human weakness is important during Lent. Believers face life’s difficulties. These struggles often leave them feeling broken and in need of divine help. [citeX] notes the health benefits of these spiritual habits. The shared nature of Lent feeds individual faith. It also strengthens the ties within religious groups. Lent leads people toward Easter. It offers hope and renewal through the promise of resurrection.(McCarthy A et al., 2020) elucidates, while individuals may strive for self-improvement through their own efforts, true fulfillment can only be realized through reliance on God’s grace. This acknowledgment of human vulnerability is vital during Lent, as believers confront the complexities of life that often leave them feeling broken and in need of divine support. Additionally, (Idler E, 2008) highlights the broader health benefits associated with spiritual practices, emphasizing that the communal aspect of Lent not only nurtures individual faith but also strengthens the supportive bonds within religious communities. Ultimately, Lent serves as a transformative journey toward Easter, offering hope and renewal in the promise of resurrection.
Lent carries deep meaning today. It asks individuals to think about sacrifice, humility, and their shared identity. Our culture changes quickly. Secular views are growing, and many people find Lenten habits difficult. These practices need deep thought and self-denial. Constant shopping often distracts from spiritual growth. Society expects instant results. This makes the struggle harder. People value quick pleasure more than deep faith experiences that change them. But Lent points to Easter. It proves the strength found in unity and God’s grace. The work on this topic reflects on living as Easter people despite cultural challenges. We must stop relying on ourselves and trust God instead. This is the heart of Lent. It shows the conflict between human weakness and God’s promise of renewal.(Pharis S, 2022). Embracing the call to relinquish self-sufficiency in favor of reliance on God encapsulates the essence of Lent, highlighting the tension between human vulnerability and the divine promise of renewal (McCarthy A et al., 2020).
Individuals reflect on the meaning of Lent. They see that this period starts a deep spiritual renewal in the Christian faith. Believers take part in fasting, prayer, and almsgiving. They face their weaknesses and trust more in divine grace. The core of Lent is not just about personal sacrifice. It highlights the need to let go of the false safety found in worldly success. This repeats a main Christian belief. True fulfillment goes beyond human effort. It comes from a relationship with God. As one text said, “Whatever we give up for Lent, we hear the call, the often difficult call, to give up most of all the reward that we can find for ourselves” . In this time of change, people welcome the Paschal mystery. They move through sorrow toward the promise of resurrection. This promise stands at the center of Christian faith and practice ..(McCarthy A et al., 2020). In this transformative journey, individuals are invited to embrace the Paschal mystery, navigating through sorrow towards the promise of resurrection, which embodies the heart of Christian faith and practice (Archives GFU, 2012)
Pressures to improve patient outcomes continue to mount on healthcare organizations. Against this chaotic backdrop, non-invasive therapies have emerged as a salve, especially in the realm of pain management.
Medical teams explore solutions that promote healing without throwing the body’s natural mechanisms out of balance. Concurrently, patients have become more informed, conducting independent research on treatments. What follows is a thorough discussion with healthcare providers before proceeding.
It is now common for those experiencing chronic pain to search phrases like ‘shockwave therapy near me’ as they explore alternatives to medication/surgery. To healthcare, this growing awareness presents both an opportunity and a responsibility. It all starts with understanding the role of emerging non-invasive therapies in better patient outcomes, something this article will discuss.
Accelerated Tissue Repair
Many non-invasive therapies, especially those that are novel, share a profound benefit in common. They can stimulate the body’s natural repair mechanisms. The best part is that this isn’t confined to masking symptoms, but goes far beyond to heal and ensure sustainable relief.
Emerging therapies can as far as enhance circulation and cellular metabolism. Care teams attuned to the benefits are better positioned to promote faster healing for patients, regardless of the disease they struggle with.
Along these lines, it’s important to keep abreast of non-invasive therapies focused on the regeneration of tissues to offer effective solutions to patients. One example of it would be shockwave therapy. Governor’s Park Chiropractic shares that shockwave treatments work by sending high-energy sound waves into the tissues. The effect is often enhanced with the use of a coupling gel.
So powerful is this stimulation that it encourages micro-trauma repair responses in the body. Likewise, other emerging non-invasive therapies can lead to the following:
Better oxygen and nutrient delivery to injured tissues
Reduced inflammation that supports faster recovery
Pain reduction
Improved Rehabilitation Care
Promoting self-sufficiency in patients for day-to-day living is the overarching aim of rehabilitation. As laid out by MedlinePlus, severe infections, chronic pain, trauma, and stroke are some of the common reasons for rehabilitation.
A range of new non-invasive therapies exists that focus on bettering rehabilitation outcomes for those with musculoskeletal injuries or post-surgical conditions. A notable example is low-level laser therapy, which, when used alongside physical therapy, can reduce pain and support recovery.
An interesting review sheds further light on this, involving 1,816 participants with about 44 randomized trials. On a positive note, low-level laser therapy reduced the sensation of pain by 60 to 70%. Jaw function was likewise improved by up to 20% in those with temporomandibular disorders.
The most long-lasting benefits were associated with longer durations (greater than four weeks) and wavelengths between 810 and 940 nm. Keeping this in view, what tactics can medical practitioners use to improve rehabilitation results? Take a look at them below:
Personalized treatment plans that match each patient’s clinical profile
Utilization of proper metrics via wearable sensors that help adjust therapy over time
A synergy of non-invasive techniques, exercise, and manual therapy for well-rounded recovery
Patient education, mainly involving information on home exercises and self-management
Greater Patient Involvement
Patient participation is regarded as a primary condition for optimal quality of care. This statement would have appeared odd back in the days. Today, it conveys how well patients adhere to their treatment plans.
A recent review of 292 studies discovered that in 58% cases, higher patient engagement was directly associated with better adherence or self-management results. Meaningful patient interactions with various therapies, even digital tools, are not negotiable.
Virtual Reality (VR)-based therapies or treatments are a good example. They allow patients to engage with exercises and get immediate feedback. With the rise in health literacy, patients feel more motivated to follow the prescribed dos and don’ts.
Both licensed healthcare professionals and nurses should work to encourage more patient involvement. The tactics listed below are paramount to that end:
Working with patients themselves to set clear goals
Showing patients their improvement via charts and apps
Verifying patients understand the ins and outs of certain therapies
Harnessing the power of technology, like wearable devices, to keep patients on track
Expansion of Medical Practice
A broader range of treatment options often results in better patient outcomes. This straightforward reality explains why healthcare providers are embracing useful modern innovations.
Established protocols may benefit from the injection of novel, non-invasive approaches. As a result, patients receive a broad array of treatment options for faster/safer recovery.
On that note, consider the example of pulse electromagnetic field (PEMF) therapy. Non-invasive and novel, this therapy has been found to reduce pain and improve both short and long-term functional capacity in patients with shoulder impingement syndrome. That’s promising in light of how painful and inflamed the condition is known to be.
This was just a singular example. The following serves as a rundown for the various ways in which healthcare practitioners can expand their practice using non-invasive therapies:
Choosing therapies based on their clinical track record for success
Staying updated on training, certifications, and best practices
Paying equal attention to exercise and patient education
Keeping an eye on patient responses and adjusting interventions accordingly for maximum benefit
For many licensed care providers, expansion may be the only way to address issues related to autonomous decision-making. Yes, diversity offers independence to determine which therapy would work best based on a patient’s condition and health goals.
Be it the field of cancer or chronic back pain, non-invasive therapies bring a whole new dimension to healthcare. Perhaps the best part is that these therapies aim to work upon the body’s innate healing mechanisms.
With relevant non-invasive therapies, the industry has the chance to rethink how care is delivered. Primary care providers desirous of expanding their care options without compromising on safety standards should look into what’s new.
Simultaneously, attention is needed towards approaches that work with the body, not against it. After all, healthcare progress is less about replacing what works but about refining it.
Author’s Bio:
Deepika is a budding content creator who enjoys exploring various niches, be it lifestyle or healthcare. With a knack for breaking down complex topics, she strives to make information relatable and accessible to everyone. During her leisure, Deepika enjoys reading novels and practicing fine arts to keep her creativity alive.
Please also review AIHCP’s Life Coach Certification program and Life Coach Courses see if it meets your academic and professional goals. These programs are online and independent study and open to qualified professionals seeking a four year certification
There are many different interpretations of verses in Scripture about God and His justice and mercy. Pending on the era of time, you also have different theologians, saints and mystics expressing within God His justice or His mercy. Sometimes, one can review readings from a particular saint that produces a harsh and fearful tribunal seat of God, while others will show a loving and caring father. Even in modern times, Christianity seems to present a dual image of God. Progressives shower one with the idea of God’s infinite love, while more conservatives display a law bound God who judges and condemns. It is very important not to overweigh one attribute over the other. If one only focuses on justice, then only a half truth emerges, which only a refocus on God’s mercy can balance into the fullness of the truth. The reality is God is both just and merciful but various interpretations from Scripture or beliefs of saints and their writings can lead one to have an imbalanced spiritual view of this. Either one that is constantly fearful, or one who is too careless with the joys of the world. In addition, how God is viewed through human lens plays a big role. Scripture presents many images of God and some can be distorted when taken too literal or for that matter entirely dismissed. Anthropomorphism is common literal device used in Scripture. In these cases God can be given many human like attributes in regards to His emotional reactions to human activity as well as images as a judge in the strictly human sense. These images need to also be properly understood in context as well as symbolism to have a greater understanding of God. This blog will look at some of these realities and attempt to balance them in proper measurement in correlation with Partial Judgement of a soul who goes to Heaven or goes to Hell.
There is a balance between God’s mercy and justice. Please also review AIHCP’s Christian Counseling Certification
God: The Loving Father of the Prodigal Son or The Fierce and Avenging Judge?
The two images above create quite a contradicting imagery but both do point to truths but when not balanced become partial truths. So many times, preachers, priests, or pastoral leaders, and even oneself finds one particular imagery of God that is superseding over all others. One’s own experience can play a large role. Spiritual individuals are attracted to certain images of God in Scriptures because it meets a need or answers an existential question that is pertinent to oneself. One’s own mental and emotional state also plays key roles in which imagery of God best fits our current need. Those who suffer from low self-esteem, or have attachment issues due to past trauma live in a state of anxiety and that state of anxiety can play a role with their relationship with God. Person’s in such mental states may have a greater fear of God, or complete imbalanced feeling of unworthiness. They may also see God as a more fierce and avenging judge. Others with a more delicate conscience or scrupulous conscience may be tormented with obsessive compulsive disorder and see God more as a judge who keeps score on the day of judgement. On the other spectrum, those who live life carelessly may need to see a parental God that dismisses foolishness and error as if it does matter what one does in life. They need a God who does not reprimand sin, but a God who only sees love. In their mind, their love of others and overall good human nature is enough-“God will not judge me but only loves me for who I am!” As one can see, these are two equally dangerous routes. Both capture an element of truth, but without each other complimenting each other, the fullness of the truth is lost.
As seen in Scripture, despite literalism or symbolism, we see a balanced approach that displays both sides of God in different books. In the parable of the Prodigal Son, one can see the untamed and complete compassion the father has for his lost son. The father never gives up loving the son and upon the son’s return, offers complete forgiveness and restoration to the son. In other imageries, one can see God as a terrifying judge who he sends souls to Hell, and casts these souls into the abyss of the wicked. The words are strong and harsh and helps illustrate the extreme disgusting nature and true evil of sin. Christ originally came as a Redeemer, but in Revelation, He is also a judger of humankind, separating the goats from the sheep. Such strong phrases as “depart from me” and “cast into Hell for the fires prepared for the wicked” all show this other side of God and Christ when judgement arrives for a soul.
Ultimately, if one wishes to truly understand God’s justice and mercy, one must understand the expression of Scripture and its aim in its full context and not individual quotes. One must be careful to avoid cherry picking of verses out of context of the chapter or theme. In addition, one must closely interpret symbolism to avoid sometimes literal interpretations that promote an anthropomorphism of God which gives Him human qualities of revenge or rage. Also, one must understand other saints or mystics interpretations of God’s justice and mercy pending on the time period they wrote and the type of language that was used. Many times as well, saints wrote in particular styles to promote one theme of God and these writings can at times seem imbalanced, especially for individuals not trained in pastoral ministry and theology. A particular saint may be illustrating God as judge and the disgusting nature of sin which can terrify a delicate soul but also at the same time promote enough self inspection and fear for a soul to change. As well, a particular saint may present writings or mystical visions that portray the totality of God’s love and the immensity of it. This may be good for a more spiritual stable soul but a message that would be dangerous for a soul who has no boundaries with sin.
In essence and answer to the leading question, God is both loving Father and fierce Judge but how one understands the true dynamics of it from a theological standpoint is essential to avoid literalistic pitfalls that can lead to scrupulous and constant fearful behavior or lax and boundless carefree behavior.
Moral Theology and Sin
Pending on one’s image of God, incomplete truths can distort one’s views on sin, but it is only when one accepts the full imagery of God, can one see the full picture of sin, self and union with God. First and foremost, Original Sin or the sin imparted on humanity after the fall of Adam, left humanity with a broken nature. The gifts of great knowledge, stronger mind and body connection and control of the passions imbedded within Adam’s character were an abilities his descendants never experienced. Through Christ’s death and application of His graces through Baptism, one again enters into full communion with God and one’s soul becomes alive through Sanctifying Grace. This however did not restore the fullness of human nature. The temporal reality and the consequences of the sin left a scar that was not wiped away after Baptism. Humanity while redeemed still was broken. While Christ reopened grace and a relationship with God through His death, the temporal reality left individuals open to sinning. Personal sin could then undo the bond of Baptism. Certain particular sins could even cut grace off from the soul. In this state without remorse, a soul again became distant from God.
St Ignatius Loyola exercises helps one examine their conscience and reflect on the justice and mercy of God
St Ignatius Loyola in his Spiritual Exercises describes sin as disgusting and deforming. Like a tumor, it tears into the soul, disfiguring it. Any sin rejects truth and the love of God. Sin is choosing self, or others over God and rejecting God’s authority. St Ignatius in his exercises challenges the soul to identify sin, to meditate on its grotesque form, and to imagine the state of a soul in mortal sin that rejects God’s love. He asks one to consider God as judge, but he also reminds us of God as father who loves. However, for whatever particular reason, in many of his meditations within the exercises, one solely focuses on God as a fearsome judge and the total worthlessness of the human person in comparison to the greatness of God. One is asked to meditate as one being a condemned criminal before a judge, as well as meditating the pains of Hell and the danger of one mortal sin. Much of this has to do with shocking the system into understanding the damage of sin and to induce a holy fear of Hell, but also a disgust for sin and a love for virtue. It also focuses to show how utterly dependent one is upon God’s grace to avoid such vile sins.
Sin is hence a great disorder and injustice itself towards God. In this way, all personal sin shares the same substance in that it damages one’s relationship with God. While all sin shares in this horrific substance, not all sins are equal in degree or depth of brokenness. It only took one sin to tear a division between God and man that Christ restored. This alone shows the vile taste of one sin and its shared characteristics but Moral theology helps one to better categorize sin, understand its objective nature, its degree, as well as the subjective interplay a sinful act has with the conscience and circumstances surrounding the agent or person committing the sin.
Personal sin is rightly divided into venial and mortal. Like human laws, degrees of severity of an offense are measured and consequences detailed through different levels of fines. A person who steals out of hunger sins differently than a person who steals from the poor. All is sin, all creates a barrier, but the level and depth of the barrier is measured by the basis of the severity of the offense. A person who commits a traffic violation remains still a good citizen despite his lapse in judgement of speeding, but an individual who murders, pillages and rapes, commits a far more grave offense to society and no longer remains a good citizen. Within the Mystical Body of Christ, offenses hurt, but the degree and multitude of the offense play a key role in whether the soul still loves God, possesses grace and remains attuned to God’s will.
Hence all sin is objectively disordered but the levels of disorder in regards to the relationship between God and the soul differ on severity. Objectively any sin remains a sin within itself. No subjective reasoning or indifference can mitigate the nature of an disordered act. The level of disorder can range objectively but the consequences of the sin can vary greatly beyond its objective label. The human act is more than a black and white event but something with multiple layers of grey. There are numerous subjective elements at play within the act of a sin. First and foremost, what is the intent of the agent committing the sin. Is the person free to act? Does the person fully intend to commit the act? In committing the act, is the person clearly articulating the acceptance of this act and all its consequences? In addition, what biological factors, psychological disorders and uncontrolled passions are at play that weaken the will? Is this act isolated or a continuous habit? Is this act done without remorse or guilt? Does one fully through this act wish to disown God? What other circumstances exist around it? Sometimes actions can become neutral that are otherwise naturally sinful-for example taking a life to defend one’s own life. What other external pressures existed? So in many cases, an objective action that is disordered possess less consequence for an individual based on other criteria.
Padre Pio saw the danger of any sin. Sin weakens union with God. Consistent sin wears one’s soul down and weakens it for greater infection. Padre Pio understood that a soul who goes to Heaven or to Hell does not randomly commit a grave sin and chooses Hell but that a soul gradually chooses Heaven or Hell over a life time. What one is when one stands before God is what one created oneself to be through a life committed and developed through virtue or vice. Habitual sin and lack of remorse leads the soul down the road of rejecting God. This is why it is critical to form a sound conscience that identifies sin as gross and disgusting and a conscience that when one does fall, immediately feels guilt and shame to confess and repent.
God’s Mercy
Sister Faustina reminds us of Christ’s infinite mercy and love
Sister Faustina is most known for her visions of the Sacred Heart of Jesus and His message of mercy. The Chaplet of Mercy as a prayer begs God for pardon and remembers the sacrifice of Christ. It repeats, “for the sake of Your sorrowful passion, have mercy on me and the whole world”. The mercy of Christ and the opportunities given by God through His sacraments seeks for all to be saved. Christ shed His blood for every soul. He shed tears for each soul lost. Many mystics claim this was one of Christ’s greatest agonies–the souls who would reject His passion and grace. Within the Sacred Heart image, Jesus’s Sacred Heart pours out beams of red and white rays from His heart. This displays His infinite mercy to sinners. Like the story of the Prodigal Son, God immediately forgives a soul that seeks forgiveness. This should not be taken for granted though. How many feel they have time to change? Instead of living in the moment, they postpone what matters most.
God’s Justice
God’s justice is referenced throughout Scripture and justice is promised to the faithful. God’s justice while merciful does not permit the wicked to go unpunished. While some may over emphasize this terrifying reality, or over humanize anger and vengeance in the Lord, many need to understand there are consequences of sin. Those who dismiss sin as trivial are led by a lax conscience that does not truly see the disgusting and foul order that sin infects the soul with. God’s standard, His commandments and His laws are not arbitrary but based in the fullness of His own essence. Something is not wrong merely by proclamation for a certain day but intrinsically is wrong for everyone and for everyday. Like evil, sin is a lack of good. It is what God is not. So when one sins, one is committing a grave injustice. Christ’s blood paid the price for sin, but as followers of Christ, we must apply the graces earned through Baptism. As followers one must adhere as best one can to the laws of God. One cannot through one’s own good works earn salvation but it is through faith in Christ and grace of the Holy Spirit that one can follow the laws of God and partake in salvation.
The Divine Judgement
In Christianity, there are two judgements. The Particular Judgement occurs at one’s death bed. The General Judgement is the proclamation and judgement upon all souls. In one’s Particular Judgement, one’s eternal fate is determined. There one sees the balance of God’s justice and God’s mercy. However as discussed early, there are many visual images in Scripture, as well as mystical writings that take these things into account.
One image, as illustrated in Scripture, displays God as judge but in a more human sense. In fact, even St Ignatius in his exercises, portrays an image of God that casts souls to Hell for their wicked deeds. This image emphasizes a strong justice display, with less mercy, but this literal image is an interpretation of that judgement. One can also from a different perspective and interpretation views God as judge from a more theological standpoint immersed in moral theology that balances God’s mercy and justice with the soul.
There are two judgements. Our immediate or particular judgement and the final and general judgement described in the Book of Revelation
One may be amazed, according to Padre Pio, how many souls who seemed evil are not in Hell, and how many souls who seemed so pious are not in Heaven. Only God knows the innermost workings of the soul. As Padre Pio also pointed out, one’s judgement before God is usually not based on one event but a life time of choices that led one to become good or evil or lovers of God, or lovers of self.
Ultimately, God as our moral standard serves as the soul’s mirror at judgement. God does not cast a soul He loves into Hell. The judgement speaks for itself. The soul as if looking into a mirror recognizes what it is in all its good and evil. It is left without distraction or excuses. It is stripped of all the noise of the world and only faced with its true reflection. Did it love God in this world or did it love self? According to Padre Pio, the soul who has rejected God is a soul who will reject God at judgement. It will acknowledge His truth finally but it will reject the truth and its implementation upon itself. The imagery of God casting a soul into Hell in some ways is hence misleading. God finds no joy in this. He loves the soul despite its total corruption but due to His standard, the soul cannot accept. Like the demons and corrupt souls before, the soul in mortal sin rejects God’s friendship, His love and companionship.
Many believe that one is saved by faith alone, but believing in God does not give one salvation. Satan and his demons believe in the reality of God but they are not with Him. The simple act of faith must be energized through the grace of the Holy Spirit to produce charity. This charity varies among individuals. Scripture attests that love can cover many sins. Ultimately, everyone is unworthy of God through one single act of sin, but it is through God’s mercy that saints and sinners alike are made worthy. So, while one’s good deeds are important choices to salvation, one must attest they are never enough. It is ultimately God’s mercy and reciprocal love that is fed through faith and grace that saves the soul before the Partial Judgement. A soul that still loves God, even imperfectly, can not cease loving God. If one loved God on earth till the end, one will love God at judgement. Hell’s greatest reality is the absence of any love. A soul at judgement who goes to Hell is a soul that refused on earth to love God and continues to refuse to love God at judgement. The soul may be well aware of what he is losing but this does not lead to contrition but only further anger , blaming and blasphemy.
Ignatius sometimes appears in his exercises to sow fear of how a soul can so easily lose God and at judgement be cast away by an angry God. There is good reason to mediate upon this, but a soul that loves God, even despite mistakes, even when some sins were in the past mortal, cannot lose God if the pattern of love remains. This entails remorse for serious sin, but God does not send a soul to Hell over a trip or fall, the soul sends itself to Hell for remaining on the ground and never acknowledging the sin or seeking forgiveness. A soul that maintains love of God, may trip and fall in life, but it always bounces back up. That same soul, no more or less than a far more virtuous soul, nevertheless shares one same common theme. No-one meets the standard of God, no mirror can display a an image that makes one worthy, whether mortal or venial, but it is the grace of God that reaches out and if love is returned, then salvation is procured. Learning to love more deeply may be required before standing fully before God, but Christ and His infinite mercy supplies the necessary gap through His blood that ultimately saves the soul.
What makes a soul choose Hell? Please also review AIHCP’s Christian Counseling Certification
Now I do not mean to dismiss the haste in which Ignatius says a soul can lose friendship with God through mortal sin, but the act of mortal sin as an objective act and its consequences upon the subjective agent can be quite differently applied. There are many souls who share sins committed on earth who are in Heaven as those who are in Hell. The difference is contrition but also charity. A soul that occasionally falls into certain sins that are classified as mortal, such as many sexual sins, does face severe danger than mere minor sins, but again all sin separates the soul from God to some degree and how the soul responds to hurting God via love matters. A soul that goes to Hell obviously exists in Mortal sin at the time of death. Obviously, these sins have defined the soul’s character and sealed its fate. Whether they were sexual sins, or sins of murder, rape, or even cases of extreme self love and unkindness to others and complete worship of this world over God, these sins represent a pattern. There are some sins especially among the deadly that represent a median line that show a point of no return or least hint towards it. Despite this, all can be converted and changed while alive, one merely needs to look at the story of St Augustine or even St Paul, but when a serious sin becomes more than an “oops” and “mistake” but enters into a habitual state of sin that renounces God and exalts self then a serious condition of darkness envelops the soul. Unlike the angels, the human intellect cannot make a decisive decision regarding to love or serve God, instead over time, the soul develops into what it will be. Hence eventually, a soul can cross a line that has led to a serious life threatening level that if one dies in it, will result in Hell. There are death bed conversions, but when one examines the life of Hitler, Stalin, or even pedofiles and sex traffickers or those consumed by lust and the sexual industry, one can see a strong difference in the deformation of the soul between one who occasionally yet with regret fell into a few serious sins as opposed to those who lived in it all the time and became committed it to the most extreme levels.
The biggest difference for the soul that chooses Hell is one that not only commits serious sin, but accepts it, loves it and live in it. I do not wish to dismiss the frightful examples of Ignatius in his exercises of one un-repented mortal sin, but I think if one understands moral theology, the psychology of the soul, as well habit in life, one is more likely to discover that most souls who go to Hell, choose it freely and not by accidentally and remorsefully tasting sin here and there. Those with broken natures who fall into serious sin as lost children can indeed if absence of remorse can find their soul in rebellion to God, but most who have conscience, who love God despite failings, rarely allow the life style to infect themselves. Instead they turn to prayer, humility and remorse. The soul that chooses Hell loves oneself over God. The soul in Hell has no charity for others. The soul in Hell sees no wrong in its actions. The soul in Hell lived in sin and embraced it. The soul in Hell does not love God, nor His laws. The soul in Hell, whether consciously or subconsciously, committed these actions with pure love and habitual opportunity without remorse. They were not merely serious sexual or selfish sins of occasion or weakness of moment, but conscious and autonomous choices of life. There was an autonomous intent and a complete disclosure in the choices it made.
These souls at the Partial Judgement are stripped of their distractions or excuses and left with the cold verdict of God. The verdict is a lack charity or love of God or others but instead complete love of self and the world. God’s verdict and justice is declared but His mercy still extends to these individuals. This may seem surprising but God still reaches out to those who even reject His love. God is still willing to forgive, but the judgement of His perfect and true self shines so brightly that such a broken and disordered soul cannot disagree with its own deformation and mutation. The soul going to Hell knows what it is and through this mirror and judgement openly rejects the mercy that comes with the justice. So, in a complete truthful image, God does judge, but God also grants mercy. In way, God’s justice does send the soul to Hell, but it is in a far different way than one’s human sense imagines it. The soul going to Hell instead rejects God and His assessment and mercy. It rejects consequences or needed remorse. It rejects even God’s mercy. This self inflicted wound is a continuation of the habitual sinful choices during life on earth that sends the soul to Hell.
On the contrary, a soul that is both saint and sinner, reflects on its image and is brought to shame and guilt but still expresses love. This soul did not die void of grace that serious sin strips from the soul but it died with grace and its most important fruit which is love. Whether more perfectly or less perfectly, a person’s love for God travels with person before the judgement of God. This love of God over love of self is the starting point of salvation for that soul. Again whether a great saint or a pitiful sinner who still finds love of God, neither are worthy of Heaven based on their individual merit due to one’s broken nature. It is solely the grace earned by Christ and one’s cooperation throughout life with grace that permits anyone to enter into union with God. The graces that energized faith and hope now fade because faith and hope have delivered what was promised. As Scripture foretells, what then remains is love. If love remains in a soul, then that soul remains in the state of grace. This soul tried its best to avoid sin, as well as serious sin, and when it fell, it humbly sought forgiveness and purged itself with tears and penance. Unlike the soul that chose Hell by its continual choices on earth, the same soul that chose Heaven chose God for most of its life and at the very end. Despite its sins, despites its failures, God and the saved soul share a reciprocal love that manifests acceptance of God’s love and will. The soul then understands clearly that it may not have loved God as much as it needed on earth but God’s love and grace has sanctified it and made it worthy.
Conclusion
Please also review AIHCP’s Christian Counseling Certification
When exploring the judgement of God and his justice and mercy, the motifs of God as judge, are applicable, and true. God is just. However, He is also merciful. He is both the God of justice but also the God of mercy as the Prodigal Son illustrated in Christ’s parable. God understands human beings are broken despite His Son’s death on the cross. He is patient, He is loving and waits for His sheep like the Good Shepherd. He does not despise the wicked but rejects their actions. He judges them based on their own deeds and decisions in life. He offers justice but also offers mercy. Ultimately, the soul dictates its future. I think it is important pending on the season or need to review both God’s justice and mercy. Ignatius will presenting a merciful God, also presents a terrifying view of judgement, Hell and the nature of sin. In addition balance this with Padre Pio’s teaching on the choice of Hell being usually more so a life time choice over time and self love and to be aware of how sin breaks us down over time. We still must be alert of individual sin in the moment, but we must remain strong and steadfast to identify it and repent from it. Sister Faustina’s Divine Mercy also displays Christ’s great love and mercy that one can find. So balance in understanding God’s mercy but also justice can help one remain steadfast in confidence of God’s love but also our own important role in keeping the commandments.
In closing, f anyone is a parent, then one understands the deep love one has a for one’s child or children. One never gives up on a child and loves the child even when the child does wrong. When the child does not seek reconciliation, it painfully hurts. Even when they walk away, the hand still extends for the child who never looks back again. While God in Scripture is seen as judge and rightfully so, it is important to see God also as a parent. Unlike some of the more vivid meditations of St Ignatius, God’s judgement does cast those to Hell but not maybe the way one envisions it, but more so as a parent who displays what must be obeyed if one chooses to return and the consequences hereafter. If the child shows just the bit of love, God, like a parent, can capitalize on that but if the child shows no love or desire to obey, and chooses instead to reject the parent, then based off his analogy, God can only watch the person enter into Hell. The terrifying reality that one sends oneself to Hell. So remain vigilant to sin, but most importantly avoid serious sin. If one falls, allow one’s conscience to identify and seek repentance. Sin is deadly and builds upon the soul and hopes to turn one serious event into continuous a life style. Maintain charity and love of God with remorse. If so, when one stands before God, it will not be a strange judge, but a loving parent.
AIHCP has numerous blogs based on Carl Rogers and his Client or Human/Person Centered Based Counseling. This blog will focus some on the general themes, goals and history of the therapy and how it set the standard for many modern day counseling techniques. Whether one belongs solely to Rogerian Counseling, or instead mixes and matches some of the philosophies and skills where needed, it remains nearly impossible for numerous Rogerian ideals not to be part of any counseling curriculum and utilized within the professional and clinical spectrum.
Please also review AIHCP’s various Behavioral and Healthcare Certifications and see if they meet your academic and professional goals.
Rogerian Psychology and Counseling- A Client/Person Centered Approach
Rogerian or person centered counseling finds its roots in counselors who express empathy and unconditional positive regard
In essence, Rogers possessed a more optimistic account of human nature and believed that helping people involved helping them help themselves and find inner healing. Instead of diagnosis, or pre-determined psycho-analysis, Roger developed a psychology and counseling that frowned upon diagnosis as well as counselor authoritarian directives but saw the counselor more as a guide and helper in unlocking a person’s potential to find happiness and balance in life. This type of counseling took some key core concepts from Adler and then became a main stay in the counseling fields since the Mid 20th Century.
Rogers taught that counselors need to help clients self-actualize to become their best self. This was accomplished through guidance that helped the person choose what is best for them. The counselor could help a person reach self actualization by helping them find congruence or genuineness with their true self. When a person was at odds with their true self or their words did not match their deeds, a counselor could help a person see this incongruence (Tan, 2022). In addition to helping a person actualize self, counselors within Rogerian schools of thought help clients understand the value of their own subjective experiences. Rogers believed that the subjective experience of a person was the most true form of self and the best way to find congruence within a person. However, the most lasting and important aspect involves the client’s condition of worth. Rogers emphasized that counselors must show deep empathy, unconditional positive regard and genuineness as core concepts in helping people (Tan, 2022). Ultimately the basis of Rogerian therapy is to not solve problems but to unlock an individual’s own solving problem abilities (Tan, 2022).
In other blogs, we discuss the critical importance of unconditional positive regard, congruence and empathy. These again are the most lasing elements of Rogerian psychology. While many adhere to some of the other concepts of subjective experience, or the role of the counselor, these three standards of counseling remain core in most counseling schools as essential elements in helping people. Beyond just being taught, these lasting qualities of the counselor also show empirically and in clinical studies strong effectiveness in helping the client. While classic Rogerian counseling swayed away from diagnosis or various therapeutic strategies, it always emphasized the importance of the counselor/client relationship. In many studies, this is the most key part whether counseling works or not. While various therapeutic strategies are essential, which ones used or not used, has more power when amplified with the counselor/client relationship.
In recent years, Rogerian Counseling has also been transformed by modifications, such Motivational Interviewing. Tan points out that this is also a person centered approach and also has many shared core elements (2022). Initially developed by William Miller, Motivational Interviewing utilizes Rogerian strategies and counselor based qualities to help clients reach goals. Tan points out that Motivational Interviewing is a collaborative approach of strengthening a person’s motivation and commitment to change. He also points out that it looks to address the ambivalence about change and is designed to help the person’s motivation by assigning goals and also exploring a person’s reasons to look for change (2022).
Interviewing involves utilizing empathy, congruence as well as unconditional positive regard, but also involves the counselor rolling with resistance of the client in a non-confrontational way. Instead helping to facilitate a picture for the client to see on one’s own to desire the change. In doing so, the counselor helps to support self efficacy and freedom of choice to fully embrace a change and work towards a goal (Tan, 2022).
Strengths and Weaknesses
Like any counseling system or psychological school of thought, one can be tied down and limited if only subject to one way of doing things with the psychological mind. This bears true with one who only utilizes psychodynamic ways without integration of other possible therapies in the cognitive fields, or for that matter approaching one from a cognitive or behavioral school of thought. Like wise, person centered psychology and counseling has strengths that can be employed, but also weaknesses when isolated and used as a the only way conducting counseling.
From a strength standpoint, the utilization of the concepts of unconditional positive regard, congruence and empathy are all staples of modern counseling. Person centered therapy also has a very optimistic view of a the human person and is rich in encouraging and helping someone find the ability to change through one’s innate abilities. It treasures freedom to choose which is the only way true change can occur.
From a weakness standpoint, it ins purest form, it avoids diagnosis and some therapies which when involving deeper trauma or pathology require more than just discussing an issue but also helping the mind heal through other proven strategies. Also, it emphasizes a complete subjective form of happiness and process of making decisions. This can lead to one’s own selfish motives, as well as choosing incorrectly in the overall scheme of life. Counselors while observing need to sometimes direct. Rogers did point to empathetic confrontation, but it needs to sometimes go farther than merely helping a person see the contradiction in one’s life but to also sometimes guide the person to the right choice. In Rogerian psychology, the counselor remains as benign a source of authority as possible in regards to direction. Many clients need guidance. This is not to assert they need told what and how to do something, but sometimes, a person needs direction. The concepts of subjective truth also come into conflict with many ideals on objective truth, as well as the person belonging to more than merely oneself but also belonging to a social construct that includes other people, as well as religious beliefs. For some, God is the source of self actualization, not the human person. For others, self actualization can become a very selfish design that ignores others and their needs. (Tan, 2022).
So again, I feel there always needs to be a measure of balance with any systems of psychology and counseling. While schools of thought exist in their purity, many counselors utilize the best of all the schools and fit it to meet the unique needs of a client.
Conclusion
Please also review AIHCP’s Healthcare Certification programs and see if they match your academic or professional goals
Carl Rogers ideas and philosophies presented to counseling were revolutionary when compared to Freudian systems. It expressed that individuals were not preprogrammed and had the innate ability to find congruence when guided by a trained counselor. The counselor was not there to solve problems but help untap the ability of the client to solve their problems. This leads to a very subjective experience of self actualization which has its strengths and weaknesses in counseling. The largest contribution of Rogers was the counseling qualities he demanded from all counselors. Namely congruence, empathy and unconditional positive regard. These elements help forge a healthy counselor and client relationship which according to studies is more important and a bigger factor in client progress than any particular therapeutic strategy employed alone. It is the counselor and client’s relationship that is the biggest factor in whether the counseling experiment works or does not work.
Please also review AIHCP’s Behavioral Health Certifications in Grief Counseling, Christian Counseling, Trauma Counseling, Crisis Counseling, Stress Management and Anger Mangement.
Meaning of existence plays a key role in understanding one’s daily trials, anxieties, stresses, as well as losses. Meaning in life can re-interpret an event for a person. From an bad event, individuals with meaning, can move forward with a better understanding and a fuller interpretation within life. Those without meaning to loss, or meaning to horrible things can fall victim to hopelessness and despair. Without an anchor of meaning, one can be swept by the various currents of life with no true direction. Existential philosophy, as well as Existential therapy, looks to find meaning in life. In this short blog, we will examine Existentialism and its influence on Existential therapy, as well as address the critical necessity of meaning in grief counseling, as well as conflicting issues between Christian theology and Existentialism.
Existentialist therapy helps individuals find meaning in loss and to also face existential anxiety. Please also review AIHCP’s Grief Counseling Certification as well as its Christian Counseling Program
Please review AIHCP’s Grief Counseling Certification, as well as AIHCP’s Christian Grief Counseling Certification and see if they meet your academic and professional goals.
Existentialist Philosophy and Therapy
Existentialist philosophy has two branches. One which encompasses a theist and sometimes Christian perspective, as well as an atheistic or nihilist branch. Philosophers such as Gabriel Marcel, Soren Kirkegaard and Paul Tillich approach existentialism from a theistic perspective, while others such as Frederick Nietzsche, Martin Heidegger and Paul Sarte present a atheistic and nihilist approach to existence. The core of the philosophy addresses humanity’s existential realities without reserve. Death, choice, freedom, isolation and meaning or lack of meaning in life are all important aspects of that cannot be ignored. Within this state of humanity, existence and its subjective and phenomenological interpretation of that existence details what a person is to be or find meaning in. There is no collective pre-existing template or essence of the human blueprint, but merely existence. As Sarte famously stated, “existence precedes essence” which at its core puts a subjective morality and choice at odds with a pre-existing objective template of reality and moral choice.
Humanity’s freedom to choose and become without fear is one of the guiding principles of non-theistic existentialist approach. As Frederick Nietzsche proposed, one must courageously drop the shackles of objective morality or the concept of God and become a “super man” who forges forward with great courage in creating one’s own essence and identity. While this is not the purpose of this blog to counter theological arguments over moral objectivity and the existence of God, this type of existentialist thought obviously places more power over one’s own decision what is good or evil.
Existentialist philosophy looks at human experience as a way one encounters life and discovers meaning. Through one’s inner self, one’s self with nature and one’s self and experiences with others. Human beings are free to relate and form one’s own meanings based on these three basic levels of existence (Tan, 2022). In this self discovery, one must be true to one’s self or authentic. It is when one ceases to be authentic with self, that pathology emerges. This becomes difficult because of natural existential dread and anxiety which in itself is not a bad thing but quite a natural thing. Within existential anxiety, one must deal with death and life, the need to act or not act, isolation versus companionship, and finally meaning or meaninglessness (Tan, 2022). A healthy existence is when these issues are faced, discussed and analyzed. When one does not dismiss these truths, as well as live authentically with oneself, then one finds a healthy balance in life.
Nietzsche presented an atheistic and nihilist perspective to finding meaning in existence
Tan lists some of the key elements of existentialist philosophy of being human. He lists first, the capacity for awareness, second, freedom and responsibility, third, creating identity and establishing relationships, fourth, searching for meaning, fifth, accepting anxiety as part of life and finally, awareness of death and non being (2022). It is when one lies to oneself and avoids these principles that pathology can occur in life. Rollo May, a existentialist therapist contends that anxiety is a critical part of life itself and now all of it is toxic but something that needs faced and addressed. Clients need taught how to face anxiety and solve the issues and problems while remaining true to oneself (Tan, 2022).
Application of Meaning in Life
Victor Frankl, a holocaust survivor, discussed in detail the grave importance of finding meaning in life, especially, in loss and suffering. He saw a deeper purpose that could help drive one beyond the mere presence of suffering. His meaning was found in love and the dignity of the human person to push beyond mere tasks and elevate them to a higher power. In this way, Frankl was not atheistic in existential thought and like others, saw the importance of spirituality as a way to find meaning. Kirkegaard also saw the importance of emptying one’s anxiety and existential angst into the grounding of all existence which is God. Hence, while to some therapists, meaning can be subjective and coming from within the person, other theistic existentialists promote the possibility that meaning can come from an outside source.
Regardless, the power of meaning is a strong driving force in interpreting life events. Frankl helped individuals find deeper meaning in his Logotherapy which utilized four primary techniques. First, he employed the Socratic dialogue, second, paradoxical intent, dereflection and attitude modification (Tan, 2022). Within the Socratic dialogue, one is directed to take a complete inventory of one’s life. This helps the person discover direction but also what matters most. Within paradoxical intent, Logotherapy looks to present the absurdity of a habit or behavior by exaggerating it. Within dereflection, the therapist helps the client see other elements of an event. In this way it hopes to utilize a type of behavioral cognitive therapy where the individual rethinks the event in different perspectives. The idea is not to dismiss or devalue the event but to approach it from different aspects. Finally, attitude modification, helps the client to change certain views or behaviors by not lamenting over the past which cannot be changed, but instead by learning from it and making good changes.
Frankl saw in humanity that all are good initially at one’s core and that it was the purpose of the therapist to help enlighten a person of one’s inner talents to utilize the goodness of the inner core. He also pointed out that life has meaning and it is one’s goal to find meaning, which usually should be in something transcending, albeit, life does not guarantee happiness even with meaning, However, it the meaning and finding that meaning in the moment that all can find direction even in the most worst case scenarios. In this way, a person retains his core, his uniqueness as well as his freedom.
Meaning and Grief
Finding meaning in existence is key but especially when loss and grief occur.
Existential philosophy and therapy plays a key role in grief and loss. Robert Neimeyer has emphasized the critical importance of meaning making in loss. Meaning is essential in understanding the nature of the loss and how the loss plays a role in the overall life of a person. Individuals who utilize meaning and find meaning not only in loss but overall life can find smoother ways to adapt to the loss and move forward with the loss incorporated into one’s life. Those without meaning struggle with suffering and loss. This was also the case that Frankl noticed in the Nazi concentration camps. Those who lost hope or meaning, even meaning in the most dire situations, would gradually fade quicker to despair and death.
Existential philosophy also demands that we do not hide from natural anxieties. In the modern world, death becomes a taboo subject, but in the lens of existentialism, it is something that should be addressed, confronted and spoken about. If we ignore death, if we ignore unpleasant thoughts of non being, then one is not living authentically according to existentialist philosophy. Existentialist therapists will help clients face the loss, understand it, and find meaning moving forward from the loss. These are all concepts and techniques that coincide with modern bereavement science.
Existentialism and Christian Counseling
As stated, there are many forms of existentialism. Some forms adapt a Christian view on life that surrenders the existential experience to God under the example of Christ. In addition, many of the concepts are concepts to use in counseling. Seeking to find answers about existence, freedom, responsibility and meaning are important concepts for the Christian but the answers from secular existentialism seeks the inner self and experience instead of the moral law of God and established dogma. In secular settings, existentialism can allow one to become one’s own god in decisions. It also tends to find most pathology from within or failure to acknowledge the existential anxieties of life and ignores many other sources of issues. Many issues stem from also biological or social settings, not just one’s imbalance with authenticity and existential anxieties (Tan, 2022).
Again, when one surrenders oneself to the autonomous self, one does not find true peace or meaning as secular existentialists would contend. That peace is through surrender of one’s anxieties to God, which is a self grounding in the Self (Tan, 2022). Kierkagaard illustrates this importance, and even Frankl addresses the surrender of self to something to a higher transcendence as something more benefitting and long lasting than merely surrender to the autonomous self. In these ways, some concepts of existentialism are useable in Christian Counseling with a strong precaution of avoiding its more secular and atheistic roots.
Conclusion
There are many good and bad aspects of existentialist therapy. Please review AIHCP’s Healthcare Certifications
Existentialist therapy while more so a philosophy than a true therapeutic concept employs meaning as a key concept for modern counseling. Meaning is essential for understanding loss, suffering and death. Existentialist therapy also helps one to not ignore the anxieties of life but to face them and find meaning in them. While some aspects of it have theistic wrappings, other elements are more atheistic in thought and look for the autonomous self and one’s authenticity to help build one’s character. This leads one ultimately to a subjective perspective on each person’s meaning of life as opposed to an objective and more dogmatic one. Regardless of belief, it has numerous benefits for counseling, in particular for Grief Counseling. Obviously, if not religious, the power of meaning in life, even if subjective, can be a powerful source for success in the world.
Please also review AIHCP’s Grief Counseling Program as well as AIHCP’s Christian Grief Counseling Program and Christian Counseling Program. AIHCP also offers a wide range of secular programs in grief but also as well in both healthcare and behavioral healthcare programs.
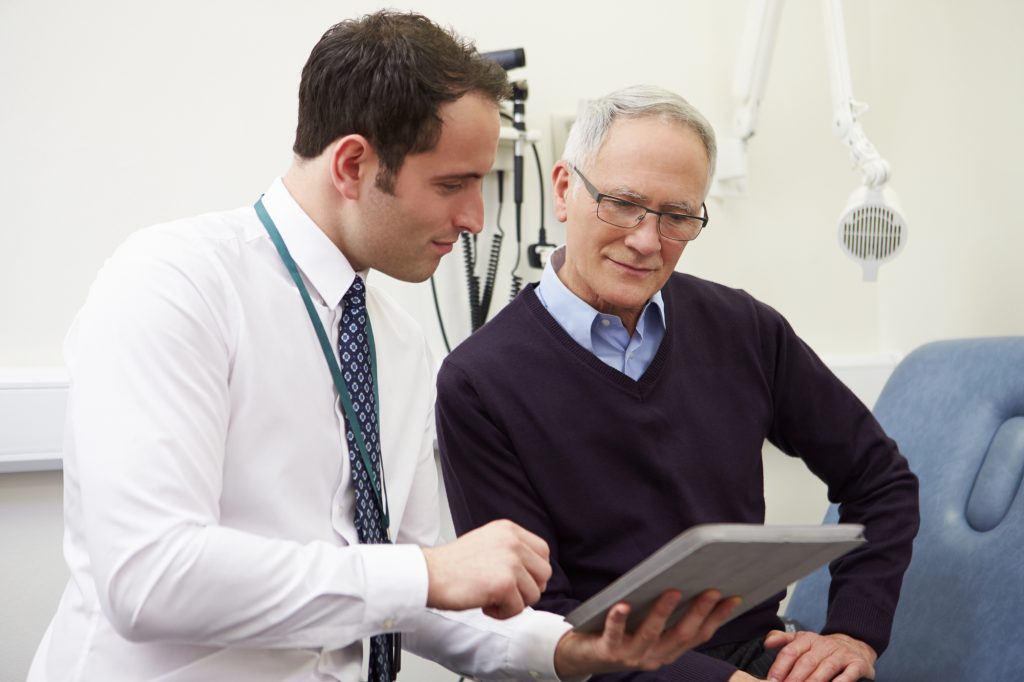 Written by Agwalogu Bob
Written by Agwalogu Bob