It is imperative within trauma informed care to be aware of and looking for signs of trauma or abuse in clients. This video looks at some signs of abuse and trauma. Please also review AIHCP’s Trauma Informed Care program, as well as its Crisis Intervention program and Grief Counseling program. AIHCP offers a variety of healthcare certification programs. Please click here
abuse
Behavioral and Mental Health Certifications: Signs of Trauma in the Population
Trauma is part of life. Bad things occur and for some the bad things are more horrific and imprinting upon the person. Estimates themselves reflect this. It is calculated that 70 percent of all human beings will experience some type of trauma that is beyond the basic losses and pains of this temporal world. In addition, 75 percent of children will experience some type of adverse childhood experience (ACE) that can negatively effect their emotional, mental, social and physical development.
While natural disaster trauma and collective social traumas leave deep marks on human beings, it is the violent and mystifying actions of evil at the hands of other human beings that leave the most devastating marks on the soul. Wars, genocides, human trafficking, sexual abuse, rape, shootings as well as being witness to horrific murders and abusive events can all leave a horrible imprint on a person, whether child or adult. While the event itself plays a key role, amazingly some individuals can process trauma and not linger with the effects of prolonged pain or PTSD. This does not make those succumb to trauma weak, or cowardly, but illustrates the reality that trauma is not just about the horrific event but also the subjective experience and the lingering effects following it. One’s genetic makeup, the social constructs and support around them, individual character and resiliency, as well as genetic and mental makeup due to past history can all play roles in how one may digest and cope trauma as opposed to another.

In states of crisis, a person suffers from disequilibrium and de-stabilization of self. The brain loses ability to handle the current situation because it overwhelms one’s coping mechanism. This leads to emotional distress and inability to cope. One is unable to think or act clearly. Those who experience severe trauma in the acute moment of it usually experience this overwhelming leaving them in the aftermath confused, lost and emotional unstable. The purpose of crisis intervention and emotional triage via emotional and psychological first aid are essential in these moments to help the person find equilibrium as well as stabilization but the efforts of long term trauma care and counseling falls under trauma informed care.
Within the population there is a high level of individuals suffering from long term trauma and PTSD. It is important for mental health and healthcare professionals to understand the signs of trauma and be better equipped to help those experiencing it in the present as well as those suffering from the past lingering effects.
Please also review AIHCP’s Trauma Informed Care, as well as Crisis Intervention and other behavioral and mental health certifications. Qualified professionals can utilize these certifications within the scope of their practice to better help those in pastoral or clinical settings of needed care.
Trauma Signs
Flight, Flee, Freeze or Fawn
The most common reactions to trauma include fight, flight, freeze or fawn (Compton, 2024 p. 105-107). The latter two have been added over the years and are equally important. In understanding human survival, these mechanisms are key in helping an individual make it through a life threatening situation. How a a person responds or does not respond does not equate to inadequacy or cowardice or acceptance of an event, but relates to numerous subconscious immediate decisions in a given situation based on subjective experiences within the person’s life. These particular reactions also play key roles in later trauma recovery because individuals may question, feel guilty or be ashamed of particular reactions.
When the body experiences a threat, the brain and body activate the sympathetic nervous system. This system releases cortisol into the blood stream and other hormones to help prepare the body for danger. The heart rate rises, blood flow increases and muscles tighten to help the body fend off the threat. In this moment of extreme stress, the brain mixed with multiple emotional responses decides to fight off the situation, flee the situation, or in some cases, shuts down the body to freeze. This is seen in nature as well. Animals will fight back, flee or sometimes freeze in utter fear in hopes of being left alone. In human beings, many of the same thoughts race through the mind. With emotion, comes intellectual thoughts based on our subjective history and experience. Can I fight this threat, if not, can I flee or avoid it, or should I freeze and hope. Many times in horror movies, we see the later. We scream at the television for the actor or actress to run or move, but the person is so terrified, he or she shows no resistance to the killer, slasher or monster. This response of freeze is referred to tonic immobility and it tied to the body’s psychological attempt to detach from reality and the danger since it has accepted fight of flight as an impossible option (Compton, 2024, p. 106). Hence some women who are raped, may completely freeze and the body shuts down while the brain experiences the fear and trauma. During this shutdown, some psychologists use other terms to explain this sensation of immobility. During the intense moments of fright of the trauma, the body may flag itself into immobility. During this intense freeze or flagging, ironically the sympathetic nervous system and its reaction releases itself to the parasympathetic system which returns blood back to the core of the body, eases muscle tension, and the body becomes almost frozen. Frozen in fright, the mental brain looks to shut down or dissociate from the trauma. In these cases, many victims may not even feel physical pain, see as clearly, or hear but they remain frozen and in some cases, even dissociate to the point of almost feeling as if out of the body and looking downward. In addition, since the trauma is so intense, the body’s coping mechanism looks to detach and many details of the assault or trauma or not properly logged. Instead, the emotional part of the brain takes over. This is also why sometimes details of survivors in regards to trauma may be not be as precise as law enforcement sometimes may wish. Finally, beyond this freezing, fright and flagging, occurs the final defense mechanism of the body which involves faint. In this, the body shuts down consciousness to the horrible ideal.
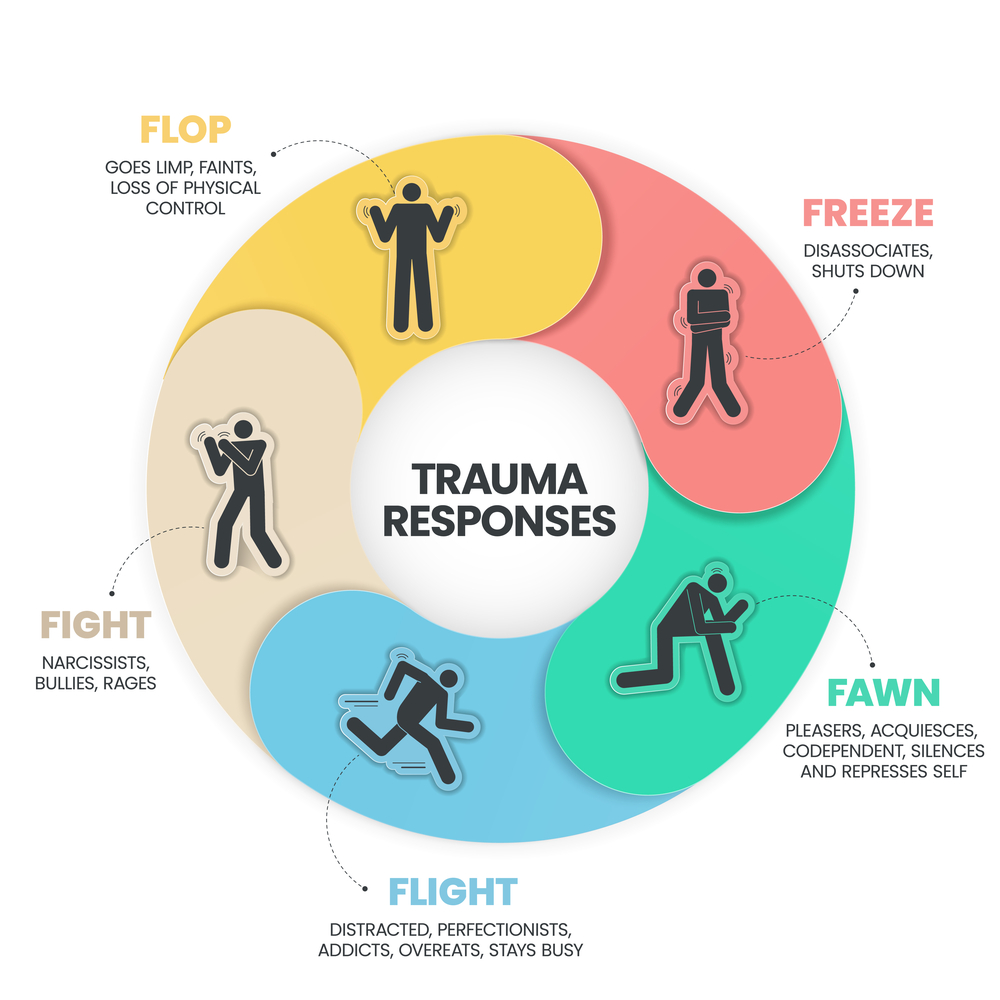
In regards to fawn, victims in an attempt to survive will work with the assailant and not resist but attempt to be be accepting of the situation. Children, and again women in assault cases, many times to survive will use this last option as a way in hopes of reducing the pain inflicted. Without escape or any hope, they succumb to the wishes of the assailant whether it involves laughing with them, or taking drugs with them, or pretending to enjoy, or partake to avoid physical injury. According to Compton, this response is completely unique to humans as a way to escape a situation in hopes of making it less worst and later survive (2024, p. 107). Some victims may consider the price of cooperating better than the price of being beaten and killed if they attempt to resist. Sometimes, pending on the psychopath or assailant, this may work in reducing injuries, while in some cases, the perpetrator injures or kills regardless. However, within the subjective mind of the victim, the call to fawn or not fawn is gamble that is made in the heat of the moment.
What later plays a role in prolonged and unresolved trauma for survivors are the cognitive distortions that can result from whichever action one chose. Those who did not fight back or flee, but froze may be hard on themselves and feel they could have saved themselves if they had just acted. A woman who did not flee a rapist, or a soldier who froze in an attack may all suffer deep remorse or regret for their actions. Yet, their responses were not so much conscious but related to inner wiring of how they would respond in this particular situation. The trauma was so powerful, they were forced to detach from the utter horrific nature of the event. Equally if not more harmful cognitive distortions can emerge with those who utilize fawning as a way to survive. They display shame and guilt and even to some extent may think they partook in it voluntarily. A woman may feel shame in laughing or accepting drugs during a rape and even doubt her victimhood but the reality is the woman entered into a survival mechanism to limit harm to self (Compton, 2024, p. 107). Counselors need to affirm the fears these individuals feel, listen with empathy and without judgement the reactions in the moment and help cognitively realign the experience with reality of “having to do what you had to do to survive”. The survivor needs vindicated in the choices made to keep him/her alive in a horrific moment no person should have to endure.
Intrusions
In addition to trauma responses and their linger effects, individuals, especially those with PTSD, suffer from intrusions. Intrusions, flashbacks, or nightmares can be triggered by simple scents, sights, sounds, or places. Due to the fact the horrific trauma imprinted upon the emotional part of the brain within the amygdala, the emotions and sounds of the moments became associated with the event. Hence even a simple backfire of a car can send an Iraq or Afghanistan veteran into a flashback on a city street. Due to the trauma, many of the normal reasoning functions of the pre-frontal cortex associated with the memory were never properly filed within the brain and processed as a healthy moment in time. Instead, the memory is raw and unprocessed as closely tied to the emotional responses of the day of trauma. In turn, a sight, scent, taste, or sound closely associated with that traumatic event can trigger a response that intrudes into the mind and takes the person away from the present. Severity of these responses vary in flashbacks but some can completely cause dissociation from the present. The person will enter into a flashback where they are no longer present. Some individuals may lose hours of the day or merely minutes pending on severity. Others will be haunted by unresolved nightmares that place the survivor back in the traumatic situation. Counselors who work with trauma survivors or individuals they suspect of past trauma will be able to identify these key signs of abuse or unresolved issues.
Hyperarousal or hypervigilance
One key sign of trauma is hyperarousal or hypervigilance. Many who suffer from trauma have a heightened sense of awareness of certain places or people. This heightened awareness activates a survivor’s sympathetic nervous system and leaves them in a state of watching or preparing for the worst. A retired soldier may watch various entrances of all escape routes or doorways even when at a simple dinner with his wife and children. A rape victim may be terrified to walk by an alley. School shooting survivors may during class time also experience issues returning to school or walking into the building. Due to the hypervigilance and the imprinted trauma, ones arousal level is so high that the thinking part of the brain cannot differentiate between the traumatic historic event and current situations that pose no threat. In addition, many completely seek shelter and protection from the public eye and seek isolation to cope with their states of hyperarousal. The person hence becomes disconnected from the present, hyper-focuses on non-existent threats, and is in a state of fear or anxiety within normal situations (Compton, 2024, p.108-109). Counselors will need to employ various emotional regulation strategies, ground techniques, exposure and EDMR therapies, or cognitive behavioral to help the person gain control of these rampant emotional memories and flashbacks.
Changed World Views and Attitudes of Survivors

Due to this new altered sense, even when not hyper aroused, the past trauma can reshape and damage previous held world views (Compton, 2024. p, 2009). Traumatic events can alter the view that the world is a safe place. Unlike many individuals in rural areas, those who frequently experience inner city violence will definitely frame a different world view from childhood onward, especially children who were never able to experience safety and security. For those who lived the American dream, those who suddenly become victim or witness to school shooting, or experience a violent crime suddenly may come to new realities that may make them challenge their worldview, faith, God, and moral framework how the world operates. Some may become cynical, others hopeless, some angry and vindictive, others may look to over-protect others because they see danger everywhere.
World views and previous held ideas lead to different reactions to situations and life itself. Some of the key points according to Compton include a lack of safety and a sense of vulnerability that did not previously exist. In addition, Compton lists a lack of trust. This lack of trust may be towards the power of God, or the power of local government to protect oneself. Many may feel forsaken and left to fend for oneself in this state of despair. Also, Compton lists esteem and defectiveness that follows trauma. Trauma survivors can exhibit negative views about themselves and doubt their worthiness to be loved after the event, or are not deserving of a good and productive post trauma life. Others may also alter views on others and stereotype races, religions, cultures and others that are associated with the trauma itself. Through this, the person is filled with anger, suspicion and bitterness towards other people who may share the same skin color or faith of the perpetrator. Compton points out that other survivors may exhibit unnecessary power and control over others or situations in an attempt to prevent the trauma from occurring again. This type of survivor may be a person who lives in constant hyperarousal and promises that what occurred will never happen again to the point of compulsion driven by anxiety. This leads to controlling even smaller aspects of life and relationships. Some may even feel erroneously partial responsible for the trauma and will look at any cost to control all aspects to avoid the same outcome. Finally, Compton lists that intimacy and how future trauma survivors respond to others and relationships can be altered. Children who experience trauma at a young age will have different attachment disorders based on trauma ranging from anxious relationship, to avoidant ones, while adults who are reshaped by trauma may experience difficulties with intimacy. A wife who was raped may be unable to have intercourse with her husband because of the violation of the sexual act in her rape. The movements or act may activate a flashback or cause intense emotional pain. Some who are not in a relationship may seek isolation and avoid attachment and at the expense of genuine human connection, forfeit future relationships due to the traumatic event (2024. p. 109-113).
Long Term Mental and Physical Signs
Trauma damages the entirety of the human person. Untreated trauma looks to numb and escape the pains through various maladaptive ways. Whether it is isolation, avoidance, or control measures, the person still exhibits the pains of trauma. Because of this, many associated with trauma become alcoholics or drug addicts hopes of numbing the pain and escaping the memories. These short term tricks however only further damage the mind and body with addiction and all the legal, financial, social, mental and physical troubles associated with it. In addition, many mentally may attempt to numb psychic pain with physical pain and self harm themselves or even idealize suicide to escape the pain. Others may utilize sex or gambling or other unhealthy way habits. Hence, those who are associated with long term and unresolved trauma are tied to depression, anxiety, physical injuries, substance abuse, and sexually transmitted diseases (Compton, 2024, p. 116).

Physically, those who deal with long term trauma even if they avoid maladaptive practices find themselves in a constant state of hyperarousal and the activation of the sympathetic nervous system. Like chronic stress, the continual state of alert has negative effects on the body, especially the cardiovascular system. Due to the constant stress, trauma survivors or life long victims of trauma find themselves with many digestive diseases, migraines and sleep issues. This leads to immune issues related to chronic inflammation throughout the body (Compton, 2024. p. 116-117). These physical issues to lead to social issues with work, education and advancement, leaving many life long trauma survivors in perilous situations beyond their trauma itself. This all has reflections on every aspect of their life and choices which can also affect other individuals negatively. When those suffer from a singular and isolated trauma, as opposed to a communal trauma, many times the individual never finds affirmation, connection, or support. These individuals, without healing, slowly rot from the vine and deteriorate. Many fall under the rug and find themselves homeless, or imprisoned for petty crimes. Others develop more severe mental illness and can lash out at others within the community.
Hence, it is a communal issue to identify trauma signs and help individuals find the help and aid they need to heal. Counselors can look for these long term mental, physical, emotional and social signs of long term trauma to better help individuals find healing via trauma informed care.
Conclusion
When signs of trauma and abuse or missed initially, or permitted to fester, the wholeness and dignity of the person erodes. Whether it is a life long series of traumas or adverse childhood experiences, or one horrible life altering event, trauma victims/survivors need help to heal. While some individuals are resilient due to numerous and multiple subjective factors, others through no fault, fall victim to PTSD or trauma induced wounds. These individuals if not helped are unable to cope in productive ways and can harm themselves, others, relationships or ruin their own careers. This overflows into society and without a empathetic and compassionate approach to help these individuals, then society as a whole suffers. Trauma Informed Care looks to identify many of the signs listed above and better help and equip individuals to find healing and healthy coping mechanisms to heal and overcome trauma. Trauma may leave a scar but it does not need to be a destructive event in the person’s life that destroys everything the person is. Instead, human beings can heal, create new neuropathways, find meaning in horror and create positive outcomes out of the darkness.

Please also review AIHCP’s Trauma Informed Care Program, as well as its many behavioral and mental health certifications for human service workers, both clinical and pastoral, as well as healthcare professionals who seek to help and make a difference for those who have experienced trauma.
Additional Blogs
Sexual Assault. Click here
Domestic Violence. Click here
Crisis Intervention in Acute Mental Crisis. Click here
Crisis Intervention Assessment. Click here
Trauma During Counseling. Click here
Resource
Compton, L & Patterson, T. (2024) . “Skills for Safeguarding: A Guide for Preventing Abuse and Fostering Healing in the Church”. Academic
Additional Resources
“Trauma and Violence”. SAMHSA. Access here
“Identifying Trauma” Center on Child Wellbeing and Trauma. Access here
Aten, J. (2020). “How to Identify and Find Help for Trauma”. Psychology Today. Access here
“Recognizing the Effects of Abuse-Related Trauma”. CAMH. Access here
Trauma Informed Care: Dynamics of Abuse and Power
Those who suffer abuse can sometimes fall through the cracks of society. Individuals, organizations, churches, establishments, or others can indirectly or directly be the cause of ignoring abuse and allowing to continue due to internal false notions, or external fears. Those in pastoral care, healthcare or mental health must be the final line of defense in identifying abuse. This may result in identifying initial abuse simply through a medical checkup, or a casual statement to the school counselor, or concerned friend, but sometimes, abuse is discovered years and years later in counseling. This is why it is so critical to make trauma informed care such a critical aspect of all counseling. So many issues emerge in life that are connected to unresolved trauma and it is so important for professionals report it as well as if within the scope of one’s practice to treat it. Counselors and pastors need to see themselves as guardians and watchers for abuse and trauma in all individuals.

In this article, we will shortly look at the nature of abuse and the dynamics of power and its role in covering abuse.
Please also review AIHCP’s Mental and Behavioral Health programs in Trauma Informed Care, Grief Counseling, and Crisis Counseling.
Safeguarding and Abuse
Compton and Patterson refer to individuals who protect the innocent from abuse as safeguarders (2024, p. 1). Anyone who wishes to promote a safe environment can be a safeguarder. Whether a observant friend, or those in pastoral ministry, or those within healthcare or mental health agencies. Everyone is called to look out for others whether the person is abused by a stranger, or a friend, or family, or within a religious institution or organization or agency. Compton and Patterson encourage others to be diligent to identify abuse by looking for signs of abuse or possible risks of for potential abuse. They emphasize in addition to looking to also listen to victims with empathy and non-judgmental attitudes that provide a safe place for them to speak. In addition to listening, safeguarding requires equipping the victim/individual/survivor with the tools to heal, build new relationships and find the necessary resources to move forward. Finally, Compton and Patterson emphasize the duty to speak out against abuse, report it and advocate for transparency within organizations that look to hide abuse (2024, p. 2).
Abuse itself is not always physical or sexual in nature, but abuse can also be verbal and emotional and in some cases, these minor forms of abuse can elevate to physical. While physical abuse is constrained to slapping, punching, strangling, burning or restraining and sexual to improper touches, exposure, unconsented recording, or rape itself, verbal and emotional abuse takes far more subtle forms. Emotional and verbal abuse can include guilt tripping, extreme jealousy, constant monitoring, name calling, insulting, sarcasm, threats, ghosting, avoidance and silent treatments (Compton & Patterson, 2024, p. 14). Spiritual abuse at the hand of a partner or even religious leader is common to control and manipulate. Compton and Patterson point out that misuse of scripture can lead to manipulation, especially to donate, or give up possessions, as well as to utilize absolute authority in other’s daily lives. When a religious leader claims undisputed authority from God without checks or balances, that leader is able to order submission to any decisions or actions he or she takes. Ultimately, the person is made to think that their service to the church or religious figure oversteps every other duty in life because the person’s salvation depends upon it (2024, p. 17).
The Power of Authority
Relationships that pend on authority and power of one over another are not partnerships but unequal relationships. When a manager, president, coach, pastor, or priest teaches, speaks, or instructs, there is a sense of power and influence over another (Compton and Patterson, 2024, p. 28). This is not necessarily a structure of evil, but an important part of organization and society, but the inner dynamics of these powers of one over another can lead to evil actions when misused. Rinaldi states, “Abuse flourishes within a system that emphasizes absolute power of leaders, encourages unflinching submission and obedience of followers and avoids meaningful accountability (Compton and Patterson, 2024, p. 26). Authority can easily be corrupted. Authority as a relationship to another carries a huge responsibility. A coach’s responsibility via his/her authority to bring out the best of his/her players, to train them, and teach them and prepare them for games. When this responsibility deviates from these norms, then his/her power is misused and tempted to abuse. Additionally, due to the existence of this relationship, it can easily blur lines and lead to potential misuse of it. Compton and Patterson point out that any leader, pastor, or manager needs to clearly understand the limits and extent of their power, as well as the consequences of misusing that power and the effects of vulnerable individuals under them within this relationship (2024, p. 29).

Those who misuse authority purposely exploit those under their control. To confuse, justify and promote compliance, spiritual leaders will utilize spiritual texts, managers will utilize company goals and professional needs, coaches will use team first mottos or personal goals as ways to contort and confuse the victim. This leads to a grooming phase where those in authority utilize their power to attract the victim outside of the arena of their relationship into other situations. Utilizing scripture, or company goals, or team needs, the perpetrator will work on altering the victim’s conscience and to make them question his/her values. Abusers with authority to cover their crime will look to normalize the abnormal and justify it. For instance, a coach may tell a player that this behavior in the locker room is normal and goes on in all locker rooms across the country. The victim who may be scared to question, or be brainwashed and manipulated into compliance may be in awe of the person, or afraid to lose a job, or a spot on the team. This leads to a cycle of abuse (Compton and Patterson, 2024, p. 31-33). The authority misused also leads to threats later. The abuser who fears accountability or prosecution will use his/her authority to terrify the abused into silence. A priest may tell a young child that no-one will believe them or that if they say anything, they will go to Hell. A politician may tell an intern, that if anything is mentioned, the person will never work in politics again. This disgusting misuse of power and abuse unfortunately happens everyday and it up to those in behavioral health, healthcare and pastoral professionals to uproot it and expose it to the light. This is an important aspect of trauma informed care!
The Dynamics of Authority and Coverup
It is important to realize that many individuals can become complicit in abuse. Some may be more direct, while others are more indirect, but the complicity still remains. Sometimes complicity at even more remote levels protect and shield the most dangerous abuses and keep victims trapped under the spell of dominance. Abusers play a part in abuse by commanding or counseling or consenting to or flattering the perpetrator. They can directly cause it or even participate within it. Others who may not abuse or condone it even play a role in allowing abuse to exist by covering it up, remaining silent, preventing steps to expose, or not openly denouncing it. These individuals in many ways are as dangerous as the abusers. While they may not abuse or have a mental illness to abuse, they care more about image or position or finance than another human being in trauma. Their crimes are an equal problem and a reason why so many institutional abuses continue within many organizations (2024, p. 12-14). Many organizations, churches, schools, or agencies utilize shame, silence, or loyalty above truth. Those who work for schools, universities, sporting teams, church positions, or organizational positions feel the pressure to protect the image of who they associate with, as well as who pays them. In addition, many within cult-like churches will look for the greater good in promoting their silence, or feel as if their salvation is threatened if they question someone of religious authority. This can lead to shame as well to encourage silence and foster the environment for abuse.

Compton and Patterson list some key concepts that lead one to complicity and silence. Unity over truth leads those within the organizational structure to silence or dismiss those who call out questionable statements, or patterns or procedures. In this case, the mission of the church or organization overplays the mission to protect individuals. This leads to the greater good motif as well as the needs of the many over the need of the one as a way to justify a crime of abuse. In addition, Compton and Patterson point out that authority over truth leads to the submission of women and children to do without question. If a coach or pastor does something morally questionable, one is told or taught to dismiss it because there is a higher reason for the crime. This leads to diluting the idea that everyone sins or no-one is perfect when comparing it to an actual crime, and then proceeding to forgive the crime as if a minor issue. Others within the organization or church who witness it, then look for reasons to justify the crime of their coach, hero, or pastor. This leads to silence and also internal coverup over an actual crime under the guise of a simple sin that no-one needs to know about and that there must be “good reason” for. In abusive church settings, the congregants are told not to gossip about a potential crime and are pushed to trust their leaders and to also only count on scripture as a source of good counsel over professional resources that would immediately report a crime (2024, p.23)
Trauma informed care probes for these signs of abuse and helps expose it.
Exposing and Preventing Abusive Systems
First, if you feel as a leader in whatever capacity you are over abusing your power and authority beyond its scope and environment, then reel it in and hold oneself accountable. If outside the office, monitor those under your care and limit relationships that are not ethical. Second, if you witness abuse, report it. Do not justify someone’s behavior, normalize it, or belittle a crime.
On a larger scale, trauma informed specialists, mental health and healthcare professionals must become advocates and face organizations that look to hide abuse. This is not only legal and the law but also ethical and moral. Sometimes it may seem whistle blowing is hurting oneself but character and maintaining one’s integrity is far greater than any position. Whistle blowing on a favorite university program may hurt the program, or reporting one’s church may feel as if you endangered the holiness of it, but we need to separate the difference between a crooked and sick individual and our favorite team or church we attend. Instead, we should be enraged that someone would abuse while wearing a collar within our faith, or if a coach would misuse the honor of coaching our favorite team to abuse others or permit abuse under his/her watch. As mentioned earlier, we must be safeguarders and this must be vocational. We are the reformers of our favorite institutions when we do report. We are preserving the future of those institutions by reforming it and removing the scum that has invaded it via reporting it. This is the mindset of a reporter. Criminals must be exposed and removed from society, especially those who misuse power, exploit the vulnerable and emotionally and physically abuse others.
Politicians, pastors/priests/bishops, managers/CEOs, and coaches are not above the institution they are in or the people they serve or manage. Their must be complete zero tolerance and complete transparency. The reforms of the Catholic Church, while slow and painful, have produced fruits with more transparency that include not only reporting but also removing the alleged perpetrator with real life consequences. Whether a company, church or university there must clear and unforgiving policies and procedures that let all those who hold authority of the dire consequences that will follow if one is guilty of misuse of power and abuse. This transparency will not taint the view of the organization but actually prove that it cares about the vulnerable and individual over crime. It takes courageous persons in dark times to stand up. Victims are the most courageous by pushing forward and telling their story. Those who report and those who seek to reform institutions are also courageous risking position, status and rejection. Stopping abuse is a community and team effort!
Conclusion
Trauma Informed Care is always looking for signs of past trauma or abuse that may stem across the life span. It looks to expose and challenge any abuser or institution that has committed the crime of abuse or misused authority. As safeguarders, mental health as well as pastoral caregivers must not only help those with trauma and abuse but also be courageous enough to be whistle blowers and advocates for the abused, forcing those who misuse authority to face justice.
Please also review AIHCP’s Mental Health and Behavioral Health Certifications. These programs include Crisis Intervention, Grief Counseling as well as Trauma Informed Care!
Additional Blog
What is Trauma Informed Care? Click here
Resource
Compton, L & Patterson, T. (2024). “Skills for Safeguarding: A Guide to Preventing Abuse and Fostering Healing in the Church”. Intervarsity Press.
Additional Resources
“Reporting Suspected Child Abuse or Neglect: A Guide for Action” Department of Health and Human Services. Access here
“The Psychology of Denial: How Abusers Manipulate, Deflect, and Deceive”. Carolyn Devers. Access here
“Abuse of power: The psychology of abusive relationships” Estaban, P. (2023). In Focus. Access here
Raypole, C. (2025). “How to Recognize the Signs of Emotional Abuse”. Healthline. Access here
Brenner. A. (2020). “10 Red Flag Warning Signs of Abuse”. Psychology Today. Access here