A closer look at spiritual direction from a Christian perspective. Please review AIHCP’s Christian Counseling Certification as well as its Spiritual Direction Program.
Author: Mark Moran
Stress Management, Grief Counseling and Trauma Informed Care: Stress & Trauma Induced Disorders
Those in the fields of stress management, grief counseling, or trauma informed care whether clinical or non-clinical are very familiar with the power of stress, loss and trauma on people. Part of existence is facing struggle and adversity. Stressors and losses, as well as trauma, negatively affect people and force them to adjust, adapt and show resiliency. Obviously, when facing a difficult loss or going through a terrible time, or even witnessing something traumatic, the mind and body reacts. This does not denote pathology but a temporary adjustment to the things, or events that occurred. It would be unnatural not to be sad or unhappy or distressed when bad things occur. It is when these things overcome one’s biology, mind and social support systems that they become unnatural. Instead of finding adjustment, one remains unadjusted through a series of biological or psychological issues that remain persistent. So while not all stress is bad, and while everyone faces loss, and not everyone faces PSTD despite severe trauma, there are cases when pathology and disorder occur that transcends the normal window of reaction in terms of severity and extreme. In these cases, individuals face biological as well as mental problems in adjusting to the issue at hand. This short blog will examine how stressors, loss and trauma can cause disorders as well as the listed disorders in the DSM-V-TR.

Please also review AIHCP’s numerous healthcare certifications for nurses as well as behavioral health professionals, including Stress Management Consulting Certification, Grief Counseling and Trauma Informed Care.
Stress, Loss and Trauma
Stress itself is not bad. It is part of life. It pushes one to face adversity and overcome it. Without the push, one would become complacent and not feel the need to improve or provide. Eustress is a term that reflects this reality (Barlow, et al. 2023). Every organism faces stress and stressors. Hans Selye, the Father of Stress Management and the effects of stress on people, pointed out that is sustained stress that gradually breaks down an organism. He listed the first phase of alarm to the stressor, the second phase as resistance to it, and finally the third phase, if resistance failed, which resulted in exhaustion (Barlow, et al. 2023). When an organism reaches a state of exhaustion, it then has biologically, psychologically and socially reached all limits to resist the stressor resulting in disease, breakdown or even death. Chronic stress usually kills over time not immediately but there can be cases when shock and trauma are so great as to cause massive strokes or heart attacks in already vulnerable populations.
Loss is a stressor in itself but loss in itself is not a pathology. Losses in life can range from the smallest things to the most important things. One can lose a job, a relationship, a pet, a parent, or spouse or even a child. These losses, like stressors, vary in degree and intensity based upon numerous subjective elements of the agent or person. For most, losses are tied to love and because of love, there is a sorrow and pain tied to any disconnection. This requires a time to heal and readjust but within normal parameters. It should not impair a person’s ability to live life. When a person is unable to adjust and the severity and length of the sadness overtakes oneself, then a disorder develops.
While everyone experiences stress and loss, traumatic events do not occur to everyone but a high portion of the population does experience them. Like any stressor, trauma while objectively seen as severe can be subjective in how a person responds. The event itself, the experience of the person and its effects play a key role in how a person responds to a particular trauma. When a trauma response activates within a person, which is natural reaction to any extreme event, the response is meant to be temporary for the moment. The survival response in the moment exists in the moment. However, when the survival response becomes a default mode of existence, then disorders such as PTSD emerge.
Mind and Body Response
When stressors or losses or trauma present itself, the body responds. The autonomic nervous systems activates the sympathetic nervous system and one enters into a state of fight, flight, freeze or fawn (Barlow, et al. 2023). The danger part of the brain, the amygdala works closely with the hippocampus and hypothalamus to prepare the body for these modes of survival. The hypothalamic-pituitary adrenocortical axis (HPA) prepares the body for fight or flight or fawn or freeze by inducing states of hyperarousal or hypoarousal to face the threat via injection of cortisol and norepinephrine into the blood stream (Barlow, et al., 2023). This tightens muscles, redirects blood to the core of the body, raises blood pressure, and heightens the person to the moment to react. After the event passes, the body returns to a calmer mode within the parasympathetic system.
When individuals are traumatized, they are unable to turn off this reaction and face a variety of issues. Long term, this can cause numerous health issues, such as hypertension, coronary issues, immune deficiencies, cancer, chronic pain and chronic fatigue (Barlow, et al., 2023).
Types of Stress and Trauma Disorders
The DSM-V-TR lists a variety of disorders directly tied to stressors, losses and trauma. They are listed in the DSM-V-TR under the chapter “Trauma-and Stressor-Related Disorders”. The manual states that those who are exposed to traumatic or severe stressful events exhibit in some cases a phenotype which is tied closely to anxiety or fear based issues (2022). In addition, these encounters lead to anhedonic and dysphoric symptoms.
Among the disorders listed, the DSM-V-TR lists Reactive Attachment Disorder (RAD), Disinhibited Social Engagement Disorder, Posttramatic Stress Disorder, Acute Stress Disorder, Adjustment Disorders and Prolonged Grief Disorder (2022).
Attachment Disorders
In regards to attachment disorders, children who experience poor caregiving at a young age develop various reactionary disorders to other caregivers which if left untreated can hinder social relationships in adulthood. This includes RAD which makes it difficult for children to form connections with others (McRay, et al., 2016). Types of attachment behaviors can be avoidant, anxious or disorganized. Each has its own characteristic which hinders a persons ability to foster proper relationships with others (McRay, et al., 2016). AIHCP offers more information about attachment disorders in other blogs that you can review at the bottom.
PTSD
In regards to traumatic response, the DSM-V-TR lists a a long list of criteria and symptoms for PTSD. It states that one must be exposed to actual or threatened death, serious injury or sexual assault in one of the following ways.
- Directly experiencing the event in person or as it occurred in others
- Learning that an event happened to a family member or close friend
- Experiencing the event or exposure to these events repeatedly
In addition, the DSM-V-TR states that the presence of at least one intrusive symptom associated with the event must manifest as
- Recurrent or involuntary or intrusive memories of event
- Distressing and recurrent dreams
- Dissociative reactions like flashbacks
- Intense or prolonged psychological distress
- Psychological reactions to external or internal cues that trigger a response
In addition, the person avoids persons, place, stimuli or things that remind them of the event to the point of impairment. They avoid past activities, portray lack of interest and diminished interest with others or the ability to experience positive emotions. The person is also negatively effected in cognitions and moods through inability to remember certain parts of the event, persistent or exaggerated beliefs about oneself or the world or meaning of life due to the event, as well persistent or distorted cognitions about the cause or consequences surrounding the event (APA, DSM-V-TR, 2022). The person will also experience issues associated with their autonomic nervous system. The sympathetic and parasympathetic nervous systems are overworked and experience hypervigilance, exaggerated responses, sleep disturbances, as well as problems with concentration (APA, DSM-V-TR, 2022). PTSD can be specified with either depersonalization, or the separation and detachment from self, or derealization or the feelings that the world around them is unreal. These symptoms must manifest for longer than a month.
Acute Stress Disorder
Acute stress disorder shares many of the similar diagnosis criteria as PTSD, but it is far less severe and lasts from day 3 to 1 month with symptoms diminishing within that time frame (APA, DSM-V-TR, 2022).
Prolonged Grief Disorder
When grief becomes complicated, it can lead to depression, prolong grief disorder or a mixture. The key difference is the locus of the melancholy is due to a targeted and specific loss (APA, DSM-V-TR, 2022). The grief itself is intense and severe and lingers, hampering a person’s ability to function in life. The duration for diagnosis is 12 months after the loss, 6 months for children (APA, DSM-V-TR, 2022). Unlike normal grief, it fails to adjust and is accompanied by intense yearning and longing for the deceased with an abnormal level of preoccupation with the loss. It includes identify disruption, continued shock and disbelief of the loss, intense emotional pain, difficulty with reintegration into life, emotional numbness, a feeling of meaningless and an intense loneliness (APA, DSM-V-TR, 2022). Of course, many of these feelings are felt within the first days, weeks and months of a loss, as well as sometimes on memorial days of the loss. This is why the 12 month deadline is so important before any type of diagnosis.
Adjustment Disorders
Adjustment disorders are tied to life stressors and losses. They illustrate behaviors or emotions that are in response to an identifiable stressor such as a loss, divorce, or loss job. The marked distress is not proportionate to the severity or intensity of the stressor (APA, DSM-V, TR, 2022). It is important to rule out natural loss, prolonged grief, as well as other cultural beliefs that can affect how people react to stress. These adjustment disorders exist within 3 months of the initial stressor
Primary Treatments
Treatment of anxiety and depression or trauma is best met with psychotherapy. No particular psychotherapy has been proven clinically to be superior or with better results as others but usually a combination of psychodynamic, behavioral and human centered counseling therapeis are key in helping individuals face their issues. Cognitive Behavioral Therapy is very helpful in helping individuals face distorted thinking and form better behaviors. Exposure therapies also exist for cases of trauma to help heal the limbic and sympathetic nervous systems. Included in this is the practice of Eye Movement Desensitization Reprocessing or EMDR. Holistic treatments that focus on meditation, breathwork and hypnosis can help the subconscious heal as well. Medication wise, numerous SSRIs, limited use of Benzodiazepines, and anti-psychotics can be utilized (McRay, et al, 2016).
Conclusion

Helping individuals with stress, anxiety, loss and trauma is part of life. In a world where bad things happen, individuals are forced to face terrible things. Some are minor, while some can overwhelm, and still, some that overwhelm can cause pathological disorders. The diathesis for disorder is based off many subjective issues ranging from biological to psychological to social to cultural and spiritual. In many cases, these life issues can be faced in a non-clinical fashion but when disorders arise, clinical help is required. It is important to remember when working in these fields to remain within the scope of one’s practice.
Please also review AIHCP’s Stress Management, Trauma Informed Care and Grief Counseling Programs.
Additional Blogs
Attachment Disorders: Access here
Complications in Grieving. Access here
Trauma Informed Care on PTSD/C-PTSD. Access here
References
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorder” DSM-5-TR (5th ed., text revision). American Psychiatric Association Publishing.
Barlow, D.H., Durand, V.M., & Hofmann, S.G. (2023). Psychopathology. An integrative approach to mental disorder (9th ed.). Cengage Learning
McRay, B.W., Yarhouse, M.A., Butman, R.E., & Kiple, C. (2016). Modern psychopathologies: A comprehensive Christian appraisal. (2nd, ed.) IVP Academic
Additional Resources
Acute Stress Disorder. My Cleveland Clinic. Access here
Blain, T. 2025). An Overview of Trauma and Stressor-Related Disorders. Very Well Mind. Access here
Sherrell, Z. (2024). Types of stress disorders. Medical News Today. Access here
Spiritual Planning Video Blog
Understanding Spiritual Planning. This video looks at how to grow in spirituality. Spiritual Directors can help guide individuals into better states of spiritual health. Please also review AIHCP’s Spiritual Direction Program as well as its Christian Counseling Certification
Spiritual Direction: Consolation and Desolation Video
Christian Spiritual Direction understands the Ignatian concepts of Suffering and desolation.
Please also review AIHCP’s Spiritual Direction program as well as AIHCP’s Christian Counseling Program
Grief Counseling: Mood Disorders and the DSM-V-TR
Mood disorders transcend the usual care of pastoral or non-clinical grief counselors. Most grief counselors deal with the natural phenomena of loss that follows a natural grief trajectory. Clinical professionals, who may also be grief counseling certified, deal with pathological issues surrounding mood. Any instability of extremes, whether due to mania or melancholy can disrupt natural life and harm mental health. Sometimes, moods can be directly affected by an acute grief or loss and this leads down a trajectory of complications due to grief, while in other cases, there is no triggering loss that causes the pathological mood. Instead it involves an in-depth investigation into the etiology of the disorder reviewing biological, genetic, psychological, social and spiritual issues to explain the condition.
The DSM-V-TR groups together a variety of mood disorders which in this blog will highlight Major Depressive Disorder, Persistent Depressive Disorder and its numerous specifiers, as well as Bi-Polar 1 and Bi Polar 2 disorders and finally, Prolonged Grief Disorder. It is important to remember that for the pastoral or non-clinical grief counselor, one should have a strong understanding of these mood disorders to help refer clients to the appropriate clinical specialists. A non-clinical grief counselor cannot diagnose or treat mood disorders but they can be trained to spot these disorders and work with clinical professionals in assuring the necessary therapy and medications are received for the client.
Please also review AIHCP’s Grief Counseling Certification, as well as its numerous other Grief Programs.
Etiology of Mood Disorders
Mood disorders find their etiology from numerous factors. Biologically, whether mania or melancholic, there is a strong connection of genetic inheritance of these pathologies tied to the neurotransmitters (McRay,2016). When the neurotransmitter, serotonin, is low, depressive states can exist. Serotonin is the a critically important neurotransmitter for mood stability (Barlow, et. al., 2023). In regards to mania, the synapses between neurons fire to fast, and a euphoric state overtakes the person. This is usually due to higher levels of the neurotransmitter norepinephrine and lower of levels of serotonin, although higher levels of serotonin can also lead to states of mania (McRay, 2016).
Depression can be caused by an internal trigger but also a stressor or external loss. Hence unipolar mood disorders can be both have a direct external stimuli as well as an internal disruption. Many times the diathesis or culmination of internal and external events that overcomes a person to the disorder can be attributed to external factors that activate it. As similar to anxiety disorders, a loss, or lack of social support in that loss, or distorted cognitive thinking can unravel a person’s natural reactions into a pathological state (Barlow, et. al. 2023).
When considering psychological etiology for mood disorders, many aspects involve self image, cognitive distortions, as well as learned helplessness in situations. When individuals engage in self negative talk and think the worst, then it can affect a person’s overall mental paradigm. In addition, when a person feels they have no control or power to prevent bad things from continuing, then the person becomes susceptible to pathological mood disorders (McRay, 2016). In addition to how one thinks, social and cultural and spiritual aspects play a key role. A person’s support system is key in any mood stabilization because it determines the foundation one has to face multiple problems before succumbing to the issue. In addition, culturally and spiritually, how one views loss can play a key role in how one reacts to loss.
As one can see, mood disorders are a complications of genetic but also psychological, social, cultural and spiritual aspects of the person. Sometimes, the mood disorder, such as depression, has a visible trigger, but other times, it is purely at the chemical level of the brain. Every individual is different and what causes diathesis and activation of a mood disorder, or even anxiety is not a simple equation but a very complex one.
Mood Disorders and the DSM-V-TR
In this blog, we will follow the order of the DSM-V-TR and how it lists and discusses the nature of mood disorders. We will primarily focus only on the above mentioned disorders.
Bi Polar I & Bi Polar II Disorder
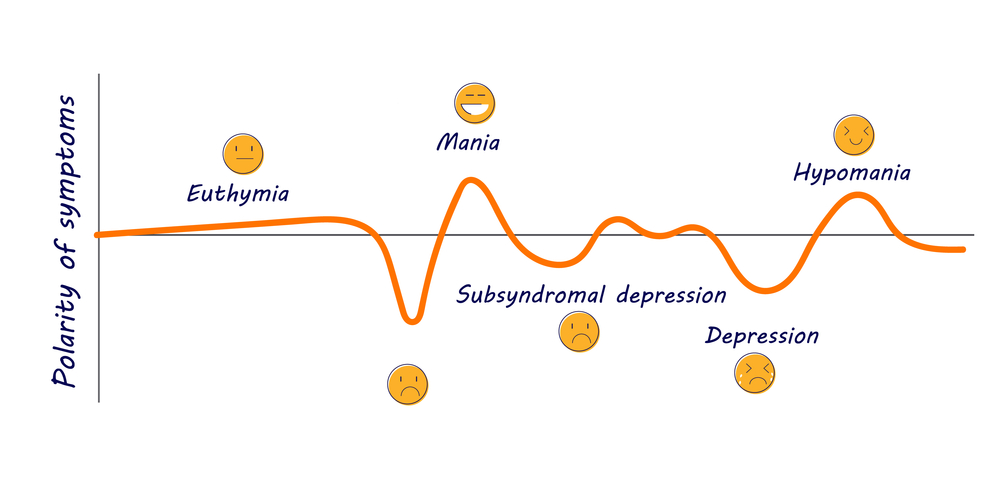
Bi polar disorders are characterized by cycles of depression and euphoria (mania) with symptoms that can greatly affect one’s ability to function in life (McRay, 2016). The DSM-V-TR states that mania is a period of abnormal and persistent moods of high levels of energy with the possibility of also irritability which lasts at least 1 week (2022). During this phase of mania, the DSM-V-TR notes these types of characteristics with three needed for diagnosis or four if the mood is only irritability.
- inflated self esteem or grandiosity
- deceased need for sleep
- more talkative or need to talk
- flights of ideas or subjective experiences that are racing through the mind
- distractibility
- increased goal directive activities that can be social, work, academic or sexually
- excessive engagement in activities with high potential for bad outcomes. Such as foolish business investments, spending sprees or sexual activitiy
The DSM-V-TR continues that these states cause severe impairment to social and occupational functioning and has no association with other psychotic, psychological, substance or medicated purposes (2022). Within itself, these are conditions for mania, which albeit rare, can exist as an issue alone apart from Bi-Polar I or II.
Ironically, Bi-Polar I does not require a depressive cycle although that is very rare for one not to be present in diagnosis. When we discuss Major Depressive Disorder and a depressive episode we will list its diagnosis as well which would be utilized with any Bi-Polar disorder.
For Bi-Polar I, as well as Bi-Polar II, the DSM-V-TR provides many specifiers since it affects individuals with so many additional subjective aspects. It can be mild, moderate, severe, possess psychotic features, be in partial remission or full remission, or also include anxious distress, mixed features, rapid cycling, melancholic features, mood congruent psychotic features or mood incongruent psychotic features, catonia, peripartum or seasonal (2022).
Bi-Polar II differs from Bi- Polar I in that there is no state of mania but there always must be a depressive state. What replaces mania is referred to hypomania. Hypomanic episodes shares the same characteristics of mania but not as severe or impairing to the individual (only 4 days as opposed to at least a week) but it still manifests a change in functioning that is not characteristic of the individual when not symptomatic (2022). In addition, the mood shift is observable by others but not enough to cause extreme distress (DSM-V-TR, 2022).
The primary differing diagnosis factor from Bi-Polar I over Bi-polar II is one has not ever been diagnosed with a true mania state ever in life.
It is important to note, some individuals who suffer from Bi-Polar mood disorders cycle more rapidly than others, with 4 mood shifts a year being considered high but there can be less cycles and individuals can move through them quickly (Barlow, et. al, 2023).
Major Depressive Disorder
While depressive episodes are part of bipolar disorders, the same criteria for Major Depressive Disorder that diagnoses an episode of depression for Bi-Polar disorders is also diagnosis Major Depressive Disorder but without any mania or states of euphoria. Major Depressive Order can find its origins biologically or also be a reaction to a loss or severe stressor. It is a unipolar mood disorder without a switching from extremes but a state of melachony
According to the DSM-V-TR depressed moods or loss of interest in pleasure must persist for periods of 2 weeks or longer (2022). Diagnostic characteristics include the following and requires five or more symptoms for diagnosis.
- Depressed mood for most of the day or nearly everyday. Feelings of sadness, emptiness and hopelessness
- Diminished interest in pleasure
- significant weight loss
- Insomnia or hypersomnia nearly or everyday
- psychomotor agitation that is observable by others
- fatigue and lack of energy nearly everyday
- feelings of guilt or unworthiness
- diminished ability to concentrate or think or make decisions
- recurrent thoughts about death, recurrent suicidal ideation without a specific plan or with a plan, as well as suicide attempt
These symptoms impair the individual in all aspects of life and are not due to any other psychological, medical or use of substance (2022).
Like bi-polar mood disorders, Major Depressive Disorder also has specifiers that dictate mild, moderate, severe, with psychotic features, partial or full remission, with anxious distress, mixed features, melancholic features, atypical features, mood congruent or mood incongruent psychotic features, catonia, post partem, or seasonal patterns (SAD) (DSM-V-TR, 2022).
Overall, Major Depressive Disorder is one of the most common mental maladies. It is considered the common cold of mental health (McRay, 2016). Women are 2 to 1 more likely to develop it, while Bi-Polar Disorder is equal (McRay, 2016).
Mentally, an individual suffering from depression faces the depressive cognitive triad that perceives negative connotations about self, the world and the future (Barlow, et. al., 2023).
Persistent Depressive Disorder
Persistent Depressive Disorder differs from Major Depressive Disorder in that is lasts longer than the normal minimum of 2 weeks but untreated can persist for months to years to decades. It is not as intense but it leads to numerous health and mental issues. Diagnosis requires a consistent 2 year period. It includes poor appetite or overeating, insomnia or hyperinsomnia, low energy, low self-esteem, poor concentration and feelings of hopelessness, (DSM-V-TR, 20220). Individuals can also suffer from both Persistent and Major Depressive.
Other Mood Disorders
Other mood disorders include Disruptive Mood Dysregulation Disorders that deal with frustration and anger outbursts, as well as Cyclothymic Disorder which does not meet criteria for mania, hypnomania or depressive episodes but still possess similar traits at a less severe level but for a period of 2 years with impaiment.
Ironically, Prolonged Grief Disorder is not associated with mood disorders in the DSM-V-TR but is a stress related disorder to acute grief which resembles depression but is a complex grief reaction. The trajectory of normal reaction to loss is distorted due to severity of the loss, or various subjective factors involving the person. AIHCP has numerous blogs on Complicated Grief as well as Prolonged Grief Disorder.
Treatments for Mood Disorders
Treatment for mood disorders should also include a integrated approach that includes medication as well as therapy. Medication only masks the problem and without life skills and abilities to understand distorted thinking, then long term healing and mental health is not possible. Also, some medications have complications which involves alternate trials and errors of different medications. In addition, many individuals feel a mental stigma when diagnosed with depression or bipolar disorders. This leads to hiding these feelings, or refusing to take the appropriate medications. This leads to continued chaos, impairment, broken relationships, loss careers, and wasted time. It is important to face mood disorders as any health condition.

Medications
Anti-depressants are utilized to help most individuals with mood disorders, especially melancholy. There are three types. First, SSRIs are the most common and most used in modern medicine. Second, tricyclic and third, monamine oxidase (MAO). The tricyclics are rarely used with the advent of SSRI’s since tricyclics had more side effects. SSRI’s stand for Selective Serotonin Reuptake Inhibitor. They prevent the transfer of serotonin from one neuron to another hence preserving a higher level of serotonin to the body to help maintain mood. MAO’s help dissolve the break down of Serotonin (Barlow, et. al., 2023). Barlow notates that 60 to 70 percent of individuals who take medication for depression experience improvement, with half of that meeting full to close recovery to full functioning (2023). A common SSRI’s include Prozac (fluoxetine). Others include Celexa, Lexapro, Luvox, Paxil and Zoloft. Sometimes, individuals must go through a regiment of different SSRI until they find the best fit and dosage necessary to manage the depression. Some need to be on SSRI longer, while others are dosed and gradually let off as needed.
Those who face treatment resistant depression can also turn to other methods to treat depression. Holistic and natural remedies under the guidance of a primary physician such as St. John’s Wort or hypericum have shown benefits as well (Barlow, et. al., 2023). Other more direct methods include Transcranial Magnetic Therapy (TMT) as well as Electroconvulsive Therapy (ECT) which directly sends impulses into the brain and neurons (Barlow, et al., 2023).
In regards to bi-polar disorders, a lithium based medication is utilized to help with mania. Lithium, a common salt in the natural environment, needs to be carefully dosed but has success with controlling mania states. It is associated with weight gain which is another reason many individuals with bi-polar disorders wish to avoid their medication (Barlow, et. al., 2023).
Psychotherapy
Psychotherapy when supplemented with medication is the best combo for treating mood disorders. It is important to fix the chemical issue but one also needs to have a strong understanding of self and ways to think differently. Cognitive Behavioral Therapy plays a key role in helping individuals reframe and rethink distortions and negative connotations about self. An individual who is depressed already has negative connotations about self, the world and the future. AIHCP has blogs about CBT and its importance as a behaviorist therapy stemming from Aaron Beck and Albert Ellis that looks to help individuals think more healthy for better behavior and mental functioning. In addition, human centered therapies which gravitate towards self esteem and congruence and fulfillment are important. Karl Rogers and his person-centered therapy looks to support the client in meeting fulfillment through empathy, genuineness and unconditional positive regard. AIHCP also has a blog to review on human-centered therapies. Finally, interpersonal skills and support is key. Individuals suffering from loss need support. An individual with better support systems can overcome different losses with more success. Some have stronger internal systems of meaning and spirituality, while others may have more family or friends or financial means to overcome loss. Basic grief counseling in these ways can help individuals become more resilient when depressed or sad.
Conclusion

Mood disorders can be stable with only one extreme or unstable and shift from mania to melancholy. They are among, with anxiety, the most common psychopathologies. Unfortunately, many individuals avoid treatment due to social stigma. It is important to find the time to take care of one’s mental health if afflicted with a mood disorder. Mood disorders can be genetic or causal but most all have solutions via medication, psychotherapy and counseling, or an integrated approach.
Please also review AIHCP’s Grief Counseling Certification as well as AIHCP’s multiple other behavioral health certification programs.
Additional Blogs
Anxiety Disorders: Access here
Grief Video: Grief: The Price of Love. Access here
Additional Resources
Bipolar Disorder. Mayo Clinic. Access here
Clinical Depression (Major Depressive Disorder). (2026). Cleveland Clinic. Access here
Dimaria, L. (2026). “Types of Mood Disorders”. VeryWellMind. Access here
References
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorder” DSM-5-TR (5th ed., text revision). American Psychiatric Association Publishing.
Barlow, D.H., Durand, V.M., & Hofmann, S.G. (2023). Psychopathology. An integrative approach to mental disorder (9th ed.). Cengage Learning
McRay, B.W., Yarhouse, M.A., Butman, R.E., & Kiple, C. (2016). Modern psychopathologies: A comprehensive Christian appraisal. (2nd, ed.) IVP Academic
Spiritual Direction and Justice/Mercy Video Blog
This video looks at justice and mercy and its application in pastoral care and spiritual direction. Emphasis is also placed on the theology behind mercy and justice and balancing it.
Please also review AIHCP’s Spiritual Direction Program as well as its Christian Counseling Certification
Behavioral Health: Anxiety Disorders
Anxiety is one of the most common mental and emotional ailments clients face. Ironically, anxiety is natural part of life. It is intimately tied to the nervous system to help push individuals. Just like stress, it can help serve individuals to meet deadlines, face problems, and persevere under pressure. To remove all stress and stressors would be a bad thing in life, as well as to remove all future angst about future issues. Anxiety itself is ontological and part of one’s being. It is part of being alive (McRay, 2016).

The DSM-V-TR defines anxiety as “anticipation of future threat (2022)”. However, when anxiety is not proportionate with the actual threat, then it becomes a malignant worry. It creates a negative mood, but the mood becomes excessive and creates a variety of somatic physiological symptoms and tensions when it becomes a disorder (Barlow, et al., 2023). So, if a student has anxiety the night before an exam, this is not reflective of an anxiety disorder, but a true reflection of potential worry of not passing the exam, however, if a student exhibits consistent worry about not being good enough to succeed in life and this filters into almost every venue of life, then one can see where anxiety can unravel into pathology.
Please also review AIHCP’s Healthcare Certification programs in mental health.
Causes of Anxiety Disorders
How one reacts and handles stressors and future problems is key to living a successful life. It is not about not feeling these interior movements, but being able to cope with them and maintain them within normal levels. There are biological, psychological and social conditions that need to be considered to explain why some individuals are more prone to anxiety disorders than others. Biologically, individuals with anxiety disorders have lower levels of gamma-aminobutryic acid (GABA) which helps keep the neurons from firing and hence keeps individuals calmer (Barlow, et al., 2023). In addition, some individuals have issues within the limbic system and its association with fight of flight. An overstressed autonomic nervous system can keep a person’s sympathetic branch more alert and on fire due to past trauma. While PTSD is now considered a trauma disorder, anxiety is still closely tied to PTSD, and individuals suffering from a variety of anxiety disorders also experience overactive sympathetic branches (Barlow, et al., 2023).
Psychologically, there are different interpretations for why anxiety exists in some and not others. Psychoanalytic schools of Freud see anxiety a severe mechanical break down of systems. Freud considered anxiety to be an internal warning sign of the ego regarding subconscious conflicts or forbidden impulses. Behaviorists considered anxiety to be due to learned behavior regarding modeling from others or cognitively through uncorrelated ideas about the self and one’s surroundings (McRay, 2016). Parents who teach their child control and predictability also help create a healthy mindset for healthier thoughts about life, coping and resiliency (Barlow, et al., 2023). In addition, parents who are overbearing and controlling, impede the child’s ability to become resilient and also incur interior fears about life that can later manifest as anxiety.
Social factors also play a key role in one’s dance with anxiety. Past traumatic events can weaken the autonomic nervous system. In addition, numerous losses, as well as interpersonal distresses ranging from divorce to loss of a family member can lower one’s ability to resist future anxiety disorders. These disorders then can effect other aspects of social functioning (Barlow, et al., 2022).
Spiritually, one’s faith can also play as a key anchor against anxiety. In fact, any world view or existential meaning in life can help one find security in times of angst. Existentialist philosophy teaches that the world is filled with trouble, loss and anxiety but it how one faces it that determines one’s control of life direction. Instead of avoidance, hiding, or fear, world views can help individuals find courage, fortitude and faith in their direction.
An integrated model for anxiety vulnerability best illustrates why some succumb to anxiety disorders and others do not. One must look a diathesis models that look at genetic vulnerabilities, life stressors, and mental and cognitive world views that all come together to overwhelm an individual. Biological vulnerabilities include inherited traits. Generalized psychological vulnerabilities include world views, such as believing the world is a dangerous and unsafe place. Finally, specific psychological vulnerabilities are what one learns from individual experience or what is taught in childhood (Barlow, et al., 2022). When an event occurs that challenges everything, some individuals may be weakened enough to enter into a disproportionate response of anxiety.
Types of Anxiety Disorders

The DSM-V-TR lists 7 anxiety disorders. Again, it is important to notate, OCD and PSTD are no longer listed with core anxiety disorders albeit they exhibit anxious symptoms and are closely related. In addition, hoarding and various picking at self disorders are tied with OCD. The manual follows life span development as its means of listing order for anxiety, as well as all disorders. It lists Separation Anxiety, Selective Mutism, Phobia, Social Anxiety Disorder, Panic Disorder, Agoraphobia, General Anxiety, and Substance/Meditation-Induced Anxiety Disorder (DSM-V-TR, 2022).
In this short blog, we will look at General Anxiety Disorder (GAD), phobias, Social Anxiety Disorder (SAD), Panic Disorders with Agoraphobia and Separation Anxiety. Please also review AIHCP’s Stress Management Program.
GAD
General Anxiety Disorder involves unsubstantiated worry over numerous dimensions of life and is not just tied to one thing, such as an attachment to one person, or how one is viewed in public. The disturbances are excessive in nature and occurring for more days than not over a period of 6 months. The individual is unable to stop or control worrying. The symptoms are tied to restlessness or being on edge, fatigue, difficulty concentrating, irritability, muscle tension and sleep disturbance. The DSM-V-TR states that only 3 or more of these symptoms are required. Key to the diagnosis is that the anxiety causes extreme impairment in social, occupational, or other important areas of functioning (DSM-V-TR, 2022). GAD is also associated with increase suicidal thoughts and behaviors. It also can have a comorbidity with depression disorders. Anxiety is usually tied at a higher percentage to women but also occurs in men.
Selective Phobias
Phobias are unrealistic reactions to things that cause heightened anxiety even without the object or thing or place present. Natural to survival and the autonomic nervous system is the reaction to fear through the sympathetic branch and its fight or flight responses. Hence fear is a negative effect within the sympathetic nervous system that alarms the body to present danger (Barlow, et al., 2023). It is important to note that many fears that become phobias are tied to natural biological and evolutional reactions. Avoiding the dark, or being careful in high places, or be cautious around potential poisonous creatures as snakes or spiders are good things but phobias hijack the sympathetic nervous system and cause disproportionate anxiety to these things even when they are not present. Phobias are coded in the DSM-V-TR according to animals such as snakes or spiders, natural environment such as heights, water or storms, blood injection-injury such bodily fluids, needles, or injections, or situational such as airplanes, elevators or enclosed places (2022).
Diagnosis involves a heightened and fearful anxiety regarding any of the listed phobias. The situation or thing must always provoke immediate anxiety or fear. These things or places are actively avoided or endured with intense fear. The fear or anxiety is out of proportion with the reality of danger. The fear or anxiety is persistent for 6 months are more. The fear or anxiety causes social impairment in social, occupational or other areas of functioning and these symptoms are not explained through other mental or substance issues (DSM-V-TR, 2022).
SAD
Social anxiety disorder is anxiety that is disproportionate based on social implications of performance, speaking, or being in social settings. Ironically, for some performers, regular social settings may not cause anxiety but for others everyday interaction in social settings, even if they are not speaking or performing can cause anxiety. Hence these individuals become extremely nervous even in school, or parties, or other events. It revolves around perceptions of how they perceive they are seen, or viewed by others. A microscopic lens is placed over every action or word they say. This may be due to fear of rejection, embarrassment or ridicule. While again, it is natural sometimes to feel some anxiety within social norms in everyday life or if performing the next day, the anxiety associated with SAD impairs functioning. It overtakes the person and causes intense somatic symptoms even upon the thought of social activity. In addition, panic attacks can associate with SAD prior to an event or during a social setting. Many sometimes will completely avoid functions, or mask it with substance abuse issues. Social anxiety disorders are more highly diagnosed with women and also children entered into their teen age years but can happen to both men and women.
Sometimes closely tied to SAD is body image. Since SAD focuses on anxiety surrounding on perceptions of others, Body Dysmorphic Disorder can play a big role especially in teens. BDD focuses on minute or even non-existent perceived flaws in the body. This subjective issue becomes a obsessive pursuit through various compulsions to alter or make better these small blemishes. For some, this disorder is then tied to SAD.
The DSM-V-TR utilizes the following diagnosis criteria. It lists marked fear or anxiety regarding one or more social interactions that expose an individual to possible scrutiny that involves conversations, social events, dates, meeting unfamiliar people, as well being observed by others. The manual notes that individuals feel they will be negatively evaluated, humiliated, or embarrassed or rejected. The social settings must always provoke fear or anxiety. In addition, the individual will look to avoid these settings and the fear and anxiety is out of proportion with the actual sociocultural context. The fear or anxiety must present itself for 6 months or more and causes intense impairment. These conditions are not attributed to other mental disorders or substances (2022).
Panic Disorders and Agoraphobia
Panic disorders are continual and persistent panic attacks. Arogaphobia is fear of public places with crowds due to the fear of possible panic attacks. Both are separate disorders but are tied closely together due to the nature of panic attacks. Panic disorder according to the DSM-V-TR is a recurrent phenomenon where an abrupt level of anxiety manifests within minutes. It can be expected or triggered or even unexpected in some cases. The attacks can occur one per week for months, or less frequent attacks separated by weeks or months. Not all panic attacks are tied to Panic Disorder since some panic attacks are tied to Social Anxiety Disorder. Panic Disorder and panic attacks cause somatic physiological symptoms that include palpitations, sweating, trembling, shortness of breath, feelings of choking, chest pain, nausea, dizziness, chills or heat sensations, paresthesias, derealization, and fear of loss of control or dying (2022). The DSM-V-TR also states that anxiety and fear over future panic attacks are followed within the month, especially in regards to the symptoms, as well as maladaptive measures to avoid future panic attacks (2022). Of course, these disturbances are not due to any other diagnosed mental issue or substance or medication.
Those who suffer with Agoraphobia fear public situations where possible panic attacks could occur and the embarrassment or issues that may occur if in a public area because of it. The DSM-V-TR lists public transportation, open public spaces like super markets or parking lots, enclosed places like theatres, large crowds or standing in line, or being alone outside of the home. The person faces extreme anxiety over these thoughts and will actively look to avoid these places to the point of impairing one’s social, professional and academic life. The fear is disproportionate, persistent and lasts for over 6 months and is not caused due to other diagnosed mental illness, substance or medication (2022).
Separation Anxiety
Separation anxiety deals with intense disproportionate fear and dread of being separated from a caregiver, loved one, or a child. It is more common in children but can also manifest in adults with children. This should not be misinterpreted for natural anxiety after a traumatic event or even a new parent, but is a persistent and disproportionate reaction that involves fear and dread of losing a loved on or something bad happening to oneself when the loved one is not present. Traumatic events, unhealthy attachments as a child, or overbearing parenting can lead to potential development of Separation Anxiety Disorder.
The DSM-V-TR states criteria for diagnosis states that excessive fear or anxiety regarding anxiety must manifest in three or more examples. Recurrent or inappropriate fear when anticipating or experiencing separation. Persistent worry about losing a major attachment figure to illness, injury, disaster or death. Worry of kidnapping, accidents, illness, or unfounded events. Refusal to go other places for fear of separation with figure. Persistent fear about being alone with the other figure. Trouble sleeping without or being away from home without the other figure. Repeated nightmares involving the scheme of separation with the figure and somatic physiological ailments such as headaches, stomach aches, vomiting and nausea stemming from the anxiety (2022). These issues must persist for 6 months in adults and 4 weeks in children and cause impairment in all social spheres of life. Again, it cannot be attributed to other mental illness, substance or medication.
Treatment

In all of these cases of anxiety, suicidal ideation can be a symptom to closely monitor. Obviously, some individuals will exhibit mild, moderate or severe and need treatments based on their individual needs. In addition, it is important during treatment to be aware of any comorbidities such as depression that may exist with presenting problem or diagnosis. It is also important to be mindful of cultural aspects that can normalize certain actions that may seem abnormal to other cultures. Finally, it is important to be delicate in diagnosis to prevent labeling and other mental health stigma (DSM-V-TR, 2022).
In clinical settings, Cognitive Behavioral Therapies (CBT) are the most utilized behavioral therapy to help the person reframe and rethink their anxieties. Some individuals with Anxiety Disorders have a recognition of of illogical thinking despite the feelings and can rationalize while others have differing levels of lack of logical thinking and are completely controlled by these thoughts. For instance, an adult with Separation Anxiety Disorder may acknowledge the improbability of bad things occurring to loved a one but still feel the anxiety while others may be completely under the delusion that something will happen. This happens also in cases of hoarding and OCD. CBT can help individuals better rationally reframe reality from fantasy and help individuals rethink what they are experiencing. For instance, someone who is facing Social Anxiety Disorder, may be able to reframe negative images and perceptions of what others are thinking into positive and more likely things, or even recognize that their perception of being the center of attention is not a reality. In regards to phobia, exposure therapies are a key way to help individuals face exaggerated anxiety. Many behaviorists believe that pathology is tied to operant and classical conditioning during childhood. How someone was raised or how their behavior was influenced plays key roles to phobias and anxiety. With phobias, new learned experiences can help reshape the neuroplasticity of the brain and how it perceives threats. Exposure therapies gradually create new experiences (Barlow, et al., 2022).
In addition to CBT and other cognitive behaviors, pharmacological treatments can help alleviate anxiety. Benzodiazaphines can help GABA levels become more stable and calm the person (McRay, 2016). Xanax, as well as Ativan can help alleviate the intense lack of calm and anxiousness and help the person find peace but it is important to note that long term use of these drugs exceeding 2 weeks or a month can lead to addiction. Hence these drugs are more for acute purposes instead of long term treatment. Many issues associated with anxiety is also tied with serotonin levels. SRRI can play a role in helping regulate mood. Paxil is a common drug used to help individuals with anxiety that can be used long term and help regulate mood (Barlow, et al., 2023).
Other holistic and natural remedies can also be utilized. Supplements for GABA under the care of a healthcare professional can be utilized as well as calming techniques, meditation, and prayer. In addition, hypnosis and EFT can also play key roles in helping manage anxiety. Please review AIHCP’s EFT Practitioner Program
From a Pastoral approach, pastoral care givers should be ready to refer clients to clinical professionals but they can also aid with coping skills, reframing, and helping individuals find meaning. For Christians, biblical approaches that tie the person to the life of Christ and how biblical characters faced anxiety can be modeling examples. In addition, how does one’s faith approach anxiety and worry? Analyzing faith and teachings can help build resiliency within the person. Spirituality is many times forgotten or swept under the rug, but spirituality plays a key role in how one thinks and feels in life. It is hence important to include pastoral approaches that address existential and spiritual explanations for anxiety in life (McRay, 2016).
Conclusion

Anxiety is natural but also the most common mental malady. Diagnosis is not a simple process but a complex one. While all these disorders differ in some degree, the primary culprit is a disproportionate anxiety response. Causes can range from biological, psychological, social and spiritual in nature. Helping others understand and sometimes helping them at a medical level is key to helping control and maintain anxiety.
Please also review AIHCP’s Stress Management Consulting Program as well as AIHCP’s multiple healthcare certifications in grief, crisis, anger, meditation, trauma informed care and spiritual counseling.
Additional AIHCP Blogs
Stress Management and Anxiety Disorders, Click here
EFT and Anxiety. Access here
Additional Resources
Anxiety Disorders. Mayo Clinic. Access here
Anxiety Disorders. Cleveland Clinic. Access here
Guy, Evans, O. (2025). “7 Types of Anxiety Disorders: Signs, Causes, & Management”. Simply Psychology. Access here
References
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorder” DSM-5-TR (5th ed., text revision). American Psychiatric Association Publishing.
Barlow, D.H., Durand, V.M., & Hofmann, S.G. (2023). Psychopathology. An integrative approach to mental disorder (9th ed.). Cengage Learning
McRay, B.W., Yarhouse, M.A., Butman, R.E., & Kiple, C. (2016). Modern psychopathologies: A comprehensive Christian appraisal. (2nd, ed.) IVP Academic
Ended Friendships Video Blog
This video looks at broken friendships whether via death or ended friendship. Please also review AIHCP’s Grief Counseling Certification.
Behavioral Health Care Certifications: What is the DSM?
This blog looks to give a short description and analysis of the DSM and its purposes and ways of classifying mental illness. The Diagnostical Statistics Manuel of Mental Disorders or DSM is a series of editions that looks to help mental health professionals diagnose mental pathology. It lists numerous types of psychopathologies and looks to classify and aid mental health professionals through the diagnostic process. It is meant as an aid not necessarily a replacement of one’s professional acumen.
Please also review AIHCP’s mental and behavioral health certifications for clinical as well as non clinical professionals.
DSM

The first edition of the DSM appeared in 1952 (DSM-V-TR, 2022). Since then there have been five editions with the most recent appearing in 2022. This edition is the revised text of the fifth edition which appeared in 2013. In 1999, the American Psychiatric Association (APA) launched an extensive evaluation of strengths and weaknesses of the previous DSMs. In efforts with the World Health Organization (WHO), as well as the National Institute of a Mental Health (NIMH), the revision began to correlate closer with the International Classification of Diseases (ICD). This led to sharing the same codes with ICD-11 instead of separate coding for mental health and diseases (DSM-V-TR, 2022). This led a better harmonization with the ICD and a regrouping of mental disorders to correlate with developmental and life span considerations of mental disorders (DSM-V-TR, 2022). The DSM-V also removed its previous multiaxial system of diagnosis which involved assessment on various axes which referred to different domains. Axis I was previously clinical disorders, Axis II included personality disorders and intellectual development disorders, Axis III included other medical disorders, and Axis IV included psychosocial factors.(DSM-V-TR, 2022). These axis are no replaced in the DSM-V with diagnosis and conditions correlated with the ICD z coding. The final axis V which included Global Assessment and Functioning was replaced by the WHO Disability Assessment Schedule (DSM-V-TR, 2022) (McRay, B., et al., 2016).
Emphasis is also placed within the new revision of cultural and social norms and the danger of abnormality being measured universally without proper context of different cultures and expression. In addition, the new revision calls for a greater focus on mental issues caused by biases and prejudices caused by race, gender, sexual orientation and culture.
The new edition also defines key terms regarding diagnosis. This includes the differences between a primary diagnosis and provisional diagnosis. Within a primary diagnosis, the diagnosis deals with the presenting issue or reason for visit. This diagnosis is based on the inpatient setting and the available information. A provisional diagnosis occurs when current information is insufficient at the time to make an official diagnosis based on needing more records or more time to unfold according to the DSM for a particular disorder to manifest (DSM-V-TR, 2022).
Important terminology for diagnosis also explains the etiology or origin of the disorder. In some cases, it will be attributed to substance abuse or medical disorders and in other cases independent mental disorder. Instead of past diagnosis with labeled disorders as organic or physical versus nonorganic or purely of the mind, current systems utilize these labels to help understand the etiology of the disorder (DSM-V-TR, 2022).
If a clinician were to review a patient’s symptoms and cross reference it with the DSM-V-TR, they would discover various headings to help one further a diagnosis. First, the Diagnostic Criteria heading lists the various symptoms that must manifest and how many the patient must possess. Second, Diagnostic Features, as well as Associated Features, Development and Course, and Risk and Prognostic Factors all provide more insight and information for the clinician to review and refresh upon. In addition to the primary diagnosis, the manual also has headings for Comorbidity and Differential Diagnosis which illustrates other possible disorders to review that are related to the patient as well as possible concurrent disorders that can co-exist with the primary disorder (DSM-V-TR, 2022).
Classification and Etiology

Many modern psychopathologies are classified according to different schools of thought but ultimately, psychopathology is a complex system. Nosology refers to the scientific process of categorizing phenomena (McRay, B., et al., 2016). Three approaches to classification involve the monothetic approach, the polythetic approach and the dimensional approach. The monothetic diagnosis is based on a “yes” or “no” classification if the agent meets the model of criteria for something or not. The polythetic which is more attuned to the true nature of psychopathology permits for a broader criteria of prototype for membership of a particular class or disorder. Criteria is more than merely pathognomonic but due to correlation, can fit some of the criteria to be included and hence creating a more heterogeneity class membership (McRay, B., et al., 2016). Dimensional models are also more diverse because they do not merely focus on qualitative distinctions between normal and abnormal but more so on a continuum of health that reviews extremes of traits (McRay, B., et al., 2016).
Most theoretical classifications fall under various schools of thought. Ultimately a multidimensional approach is critical and is what the DSM utilizes. Among theoretical perspectives there are biophysical theories which emphasize physiological factors that determine psychopathology. Included also are intrapsychic which primarily assume psychological factors, phenomenological factors which stress experience and perception, and behavioral theories which focus on how a person’s learning and personality was determined by reinforcement (McRay, B. et al., 2016).
The primary foundations for all mental illness finds itself in four broad models of psychopathology: Biological, psychosocial, socio-cultural, and spiritual. Biologically, mental maladies can be due to genetics and physiological factors. Psychosocial reviews the formation of psychopathy from the numerous branches of psychology. Whether from a psychoanalytic perspective, or a behavioral perspective, or even a humanistic perspective, psychopathology and illness is an expression of underlying personality dynamics, environmental factors, internal thinking processes or learned habits that create pathology (McRay, B., et al, 2016). The socio-cultural pinpoints where some psychopathologies can emerge due to cultural and family aspects of development and how they play a role in a person’s mental health. This includes the role of social labels and roles, as well as social connections and support play in the development of one’s mental health. Finally, spiritual models look at the power of identity, meaning and existential realities and how these spiritual practices help or hinder a person’s mental health (McRay, B., et al, 2016).
Caution when Utilizing any Diagnosis
The DSM-V-TR when used by untrained professionals can be dangerous. Also, even for trained individuals, it is important to understand that the DSM-V-TR despite based on a wealth of knowledge, empirical research, as well as multiple health organizations is still limited in diagnosis. According to McCray, DSM V categories are more descriptive than explanatory. He also points out that diagnostic labeling needs to be done with sensitivity and care to avoid damaging the self worth of an individual (2016). Ultimately, the field of psychotherapy is not an exact science and false diagnosis can occur. While the most current DSM is the premiere resource, it is only as reliable as the trained user utilizing and applying it. Humility and thoroughness in assessment and diagnosis is key, as well as a Rogerian sensitivity in discussing an mental disorder. A person should not be a seen as “this” or “that” but a person exhibiting traits of “this” or “that” or suffering from “this” or “that”. This prevents labeling, mental stigma, and including the identify of the person with the disorder itself.
Conclusion

The DSM-V-TR is the most current edition of the DSM at the time of this blog. As science and the medical field discovers more, new editions will emerge. As new strategies and ways of viewing mental illness emerge, new editions will incorporate them as well. In the meantime, those in behavioral health and the clinical side must adhere to the best and most current ways of understanding, diagnosing and treating mental health.
It is important to remember that non-clinical members of AIHCP who may be certified are not entitled to diagnosis and treatment. Individuals in grief counseling who are not licensed need to refer clients to the appropriate professionals. Please also review AIHCP’s healthcare certifications for both clinical and non-clinical counseling in grief, stress, anger, crisis, trauma informed care, spiritual and Christian counseling programs.
References
McRay, B., Yarhouse, M., & Butman, R. (2016). Modern psychotherapies: A comprehensive Christian appraisal (2nd Ed). IVP Academic
DSM-V-TR. Access here
Additional AIHCP Blogs
Diagnosing Psychopathology. Access here
Additional Resources
DSM-5. Cleveland Clinic. Access here
First, M., et al. (2022). DSM‐5‐TR: “Overview of what’s new and what’s changed”. World Psychiatry. May 7;21(2):218–219.
doi: 10.1002/wps.20989
Fritscher, L. (2026). Advantages and Disadvantages of the Diagnostic Statistical Manual. VeryWellMind. Access here
APA. DSM-5-TR Online Assessment Measures. Access here
Christian Spiritual Direction and Counseling: Analysis on Ignatian Discernment of Spirits and Election
This is a short blog that will analyze and clarify St. Ignatius’ concept and semantics regarding desolation and consolation and their use in discernment of spirits and election or choice. This is a general blog for any interested reader as well as a synopsis for those in AIHCP’s Christian Counseling or Spiritual Direction courses, as well as those enrolled in Ignatian Spirituality.
Please also review AIHCP’s Christian Counseling Certification.
Introduction

For those in the Spiritual Direction Program, consolation and desolation are universal Christian terms but primarily stemming from the Catholic tradition. So for those who are Protestant or from non-denominational faith traditions, do not feel intimidated. These concepts can be applied and should be applied in spiritual direction regardless of Christian denomination. None of these concepts deal with any dogmatic dispute between denominations of Christianity and can be universally applied to Catholic/Orthodox and Protestant traditions. These concepts are extremely helpful in guiding souls as well as helping alleviate spiritual times of suffering.
I would like to point out that the terms desolation as well as consolation can be utilized more generic in sense regarding mood of the soul. St Ignatius points out that in consolation, the soul’s interior is aroused with spiritual sweetness from the Creator and inclined to the will of God via this good spirit. In contrast, he states that desolation is a time of inner turmoil and restlessness of the soul when it is inclined away from God and influenced by a false spirit.
This may seem confusing when we hear the term consolation and desolation its pure emotional semantic meaning. In cases of other mystics, such as St Teresa of Avila, consolations are times when the soul feels God’s presence and desolations are when the soul does not feel God’s presence. I myself in a video reference the term in this more simple format. Ignatius would refer to desolation in this sense as difficult consolation because the soul is still inclined towards God and pushing forward while in Ignatius’ concept of true desolation, the soul is falling away from God, albeit not necessarily in a state of sin but one of spiritual apathy. St Teresa of Avila refers to simple desolation as more spiritual aridity, while Ignatius seems to refer to it more as spiritual apathy. These are big differences but I wanted to notate this when reading the Ignatian texts. Again for Avila, it is a simple emotional state, for Ignatius it is more than just mood but also a disposition of the soul that comes and goes in different phases and periods of times. So there is a distinction between Avila and Ignatius between an emotional state and a spiritual state in regards to the word. Again, desolation is not in itself sinful but it can lead to sin and bad habits because it is guided by false spirits and interior dispositions.
What are Consolations and Desolations?
Consolation
A consolation can be considered an emotional state of intense union with God but also a spiritual state of union with God that is in sync with God’s will and laws. According to Thibodeaux, it can be dramatic as well as placid in nature (2020). In a dramatic state, the soul experiences a moment with God that is overwhelming and exciting to the soul and the body’s senses. It is uplifting and warm. One in a state of placid consolation is not a in a current state of intense excitement but a consistent balance. In comparison, consider dopamine and serotonin. Dopamine as a neurotransmitter produces an intense edge, while serotonin as a neurotransmitter produces stability of mood. I think this best explains this balance between dramatic and placid consolation.
It is important to remember that consolation itself is gift. It cannot be earned by praying a certain way or meditating but is a gift from God. He grants it to whoever He desires. We should then be grateful and thankful to God when He chooses to gift the soul with more intense presences. St Teresa of Avila expresses different states of reward in prayer, namely the Prayer of the Quiet when God reveals Himself without effort on the part of the person, as well as Prayer of the Union, when the soul also receives an unexpected and unearned gift of a deep unitive gift with the Divine. These are all greater examples of consolations. Ignatius also speaks of unexpected and memorable spiritual experiences and refers to them as Consolations without Previous Cause (Thibodeaux, M., 2020). This is similar to extraordinary spiritual experiences that the soul is granted by God.
Strangely enough, even during consolation, the soul can feel what St Teresa of Avila would refer to aridity. St. Ignatius does not refer to this state of aridity as a desolation but a Difficult Consolation (Thibodeaux, M., 2020). In this, Ignatius points out that the soul is still directed toward God and is not facing a desolation that puts the soul out of sync with God. Instead, while still experiencing aridity, the soul still is orientated toward God.
Desolation
In contrast, desolations, according to St. Ignatius, are darker moments of the soul’s spiritual phases. It is time associated with anxiety, depression, and inclination towards false spirits and bad habits. The soul is not in sync with God. These false spirits can but are not necessarily even demonic in nature but more natural inclinations of humanity’s fallen nature. Energies or inclinations towards the world, or particular vices that bring the soul downward away from God towards other sources of “completeness”. This state does not designate sin in itself but can lead to sinful situations and sinful aspirations.
Like consolations, the desolation can be dramatic or placid in nature. They can be an intense anxiety or merely a tiresome and gradual decay of the soul’s spiritual life with God. In other cases, there can be False Consolations, where the soul feels it is following God’s calling but in reality is fulfilling one’s own desires and needs (Thibodeaux, M., 2020).
The Spiritual Life: A Spiritual Rollercoaster
Spiritual life is filled with waves of consolation and desolation, as well as emotional “consolation” and “desolation”. Life happens and things can occur that make us very happy or very sad or angry. These life events can steer us closer or away from God through certain phases of life. The loss of a child, or a parent, or any loved one can lead some individuals into a desolation against God which includes anger and resentment. Likewise, individuals can go through numerous loses and pains in life, but still remain in sync with God, but feel truly empty and sad over such losses. These are natural bio-rhythms. Like the body, the soul also goes through natural ups and downs. What is important is to orientate one’s self to never lose sight of God even in the rough times, even in times we do not feel His presence.
It is also crucial to understand the psychological components of desolation as well as consolation. Psychotherapy tends to separate soul care and mental health but both are uniquely tied together. This does not mean clinical depression should only receive spiritual advice but it does mean within all melancholy, there is also a saddening of the soul. States of depression can distort thinking and value of self as well as one’s relationship with God. Desolation can make one doubt one’s love from God, as well, as to hate oneself for past sins and feel a lack of forgiveness. These deeper states of desolation leave the soul out of sync with the Divine and can lead it to other maladaptive practices to find solutions from the pain. So, spiritual desolation itself can be a dark time, but it is even darker when tied to mental health issues. Spiritual Directors, while understanding the union between soul and mind, but also understand the need to refer individuals for psychological help when signs and symptoms of clinical depression emerge.
Guiding others through Spiritual States

Thibodeaux discusses multiple applications of spiritual direction through different states of consolation and desolation.
In consolation, he lists numerous points but importantly, one needs to remember to encourage humility and thankfulness in these states, but also to prepare one for future desolation. In times of consolation, he recommends that individuals journal the good times so when tougher times arrive, they can fall back on these emotions and feelings as a spiritual anchor. He also points out that it is during these times that one has the most clear head to make elections or decisions (2022). Ignatius believed during consolation, the soul is able to understand God most and be able to make decisions. Decision making is difficult enough. Life decisions are not easy mathematical equations but require our whole being partaking in it. When one’s conscious and subconscious –mind and soul–find God’s presence and can hear His voice, then elections can be made. However, like any dopamine affect, it is important to reflect also on these decisions which are indeed well-founded, but once a more stable mood is restored, one can reflect on the extraordinary insight God has given. This is why Ignatius, while dictating the validity of election in this state, does think it is wise for immediate action on it until it is reflected upon. Ignatius teaches that discernment also involves feeling the spirits of the movement. In consolation, these are genuine, but one must be certain of the genuine experience. This is especially true if one experiences an extraordinary spiritual state, as as Ignatius would refer “Consolation Without Previous Cause”. In this state, the soul, as well as the body feeling in the intake of dopamine and happiness, should wait a short period to stabilize mood wise. In this way, the intellect can share in the evaluation of the message before acting in haste (Thibodeaux, M., 2022). Spiritual Director help souls recognize true consolation over false consolation and also help souls discern the messages and movements of the soul during them. They help the soul understand when it is good to make a choice or election when sound mind exists that correlates with the valid message of a consolation.
In regards to desolation, it is a time for even more renewed prayer and to remind the directee that acting on any impulses or changes during this time is dangerous. A soul in desolation, even in troubled consolation, should not act due to the variety of emotional blinders. Until the blinders are removed, the soul could be influenced to poor decisions. For instance, many depressed individuals turn to maladaptive coping or choices for a quick fix. They will try to feel good by merely making a move in life to alleviate the desolation. Spiritual Directors must utilize empathy, patience, and unconditional positive regard to these souls. They need to help them cognitively reframe false assumptions or low images of self that have influenced them via the false spirit. Psychology gives many tools to help people rethink about themselves. Cognitive Behavioral Therapy teaches individuals that bad thoughts create bad self image and behaviors associated with those thoughts. It is important to reframe these thoughts or images and help the directee re-evaluate in a different light.
Another important thing to consider in desolation is the movement of the enemy within the soul. A soul that begins to change itself will be met with loud noise and anger from the enemy. Those looking to re-orientate themselves will face stiff resistance that can produce anxiety and depression. It is not only a spiritual battle, but also a psychological rewiring of neuropathways that are tied to bad habits of the past. Likewise, the soul who is muddied and stuck in desolation quietly acquiring bad habits of spiritual sloth, or any other vice, will form habits but the approach of the enemy will be far more quiet and less disturbing. Only till the soul pulls away, will the enemy become loud again with persistence in pushing bad habit and vice.
It is of no wonder then that Ignatius emphasizes the danger of making an election or drastic decision in this state of being. Only until balance or equilibrium is restored with God can the soul regain composure to make healthy and good decisions that are aligned with God. Spiritual Directors who work with souls in deep and acute desolation need to help the soul again find balance and then exhibit extreme patience with the individual as he or she again looks to hear God and answer Him.
Desolation is obviously a natural part of life. It can be caused by life itself and the sorrows of this world. It can be deep and disorientating but it does not necessarily mean the soul needs to lose sight of God. Those in desolation, or even simple aridity, are called even more so to daily prayer, even if there is no warmth or sense of happiness. Eventually, the soul will come out of desolation, but again, those with psychological issues, with also require professional mental health providers to help them.
Why would God permit this? First, it is the natural state of humanity. In regards to abandonment, Christ Himself felt alone or desolate, albeit, never out of align or not in sync with God, since He is God incarnate, but this does not mean He did not sense or feel within His human nature, the fear, anxiety and angst of life. In the Garden, He wept blood, and on the cross, He felt forsaken. So, whether in desolation, aridity, or troubled consolation, the emotions and feelings associated with it are part of the natural world. Jesus teaches us how to fight them.
God also uses these moments as teaching moments to train the soul on its dependence on God. St. Ignatius points out that the soul can become proudful of its own accomplishments in false consolations, or may feel consolations of intense proportion are earned or deserved. A soul that continues to fight, sees its own humility and dependence upon God can learn much through desolation and aridity.
Conclusion

I hope this clarifies some of the semantics regarding desolation and consolation that we hear in spiritual states of life. Obviously this is more so focusing on St. Ignatius and the Thibodeaux text in understanding consolation and desolations in Spiritual Direction and how to guide souls through these states to make better choices.
Please also review AIHCP’s Spiritual Direction Program as well as its Christian Counseling Program
Reference
Thibodeaux, M, SJ. (2022). Ignatian Discernment of Spirits for Spiritual Direction and Pastoral Care: Going Deeper. Loyola Press.
Additional AIHCP Blogs
Vocation and Discernment: Access here
Desolation and Affliction. Access here
Additional Resources
Peoples, I. (2022). “Jesuit 101: Consolation and Desolation”. The Jesuit Post. Access here
“Consolation and Desolation”. Ignatian Discernment Institute. Access here
“Discernment: Consolation and Desolation”. Loyola Press. Access here